Introduction
Population aging is one of the most significant trends in the 21st century. It is generally expressed as older individuals forming a large share of the older population.1 Two main factors of population aging are an increase in life expectancy and a decline in fertility rates. 1 Life expectancy at birth is projected to continue to rise in the coming decades in all major regions of the world. 2 Being a very diversified country with different strata of populations, India may face problems differently in its rural and urban regions.. In India, many of the nutritional factors developed from lifestyle and behavioral risk factors, are found to be associated with the prevalence and contributory for developing communicable diseases among the population.3
Behavioral risk factors constitute a major contributory factor leading to nutritional problems associated with non-communicable diseases. 3, 4 A study conducted in one of the capital cities in Kerala demonstrated that smoking, alcohol consumption, inactivity, stress, unhealthy diet, along with low socio-economic background were major risk factors associated with the development of chronic diseases, with more than a quarter of females having obesity. 4 The demographic and epidemiological transition in low and middle-income countries have brought a major shift in the nutritional habits of adults and have contributed to an increase in overweight and obesity resulting in chronic conditions, metabolic disorders, cognitive disabilities, and various cancers.4, 5
Prevalence of malnutrition can vary from country to country and the risk factors leading to it demonstrates factors associated with lack of knowledge and associations with their sociodemographic variables. A prevalence study conducted among randomly selected 245 older persons(age > 60 yrs) in a rural block area of South India, 4 shows that malnutrition is present among 14.3% of adult population and also a risk among 44.1% of them.5 Prevalence of underweight, overweight and obesity is reported in 2.0%, 34.0% and 17.0% respectively among 300 elderly people residing in South Africa.6 In addition, nutritional deficiencies were also commonly reported among elderly in that study who didn’t meet the reference intake of protein, iron, zinc, potassium, calcium and vitamins B1, B12 and C.6 Many elderly skip meals or have inadequate intake of micro-nutrients which are not reported or underreported, and also the intake in terms of vegetables and fruits are less than satisfactory.4 In a study carried out in Ernakulam, Kerala, among the old age home residents demonstrated that economic dependency, social deprivation, and change in behavior towards diet and health care make the elderly more vulnerable to malnutrition and ill health.7
Another study that supports the present study was conducted among 3871 older adults in nine states of India, and anthropometry was done for all of them. A total of 2138 older adults were covered for dietary assessment. The result shows that consumption of all the food was below the recommended daily intake and the inadequacy of intake was high concerning leafy vegetables, milk and milk products, fat and oils and sugar and jaggery. Similarly, adequacy of intake of micronutrients such as vitamin A, iron, riboflavin, and free folic acid was high among both genders. Also skipping meals, especially supper, was common among older adults which can lead to malnutrition among the older adults. About 9.6% of the elderly ate supper sometimes, while 13.7% didn’t eat their supper. 8
Studies conducted all over India to assess nutritional risk factors in a population of community-dwelling older adults in Kolkata, India the result showed that the prevalence of undernutrition was 8.8% in females and 4.8% in males. 9 Another study conducted in Thiruvananthapuram, Kerala among 245 older persons to assess the prevalence of malnutrition in an rural area showed that 14.3% were malnourished and 44.1% were at risk for malnutrition. 5 In a study carried out by Abraham et al., among 129 older adults in community, 2 it was noticed that education status, occupational status, and monthly family income were significant factors affecting the nutritional status of older adults. The same study reported that about 11.6% of the people were malnourished, and 46.5% of them were at risk of malnutrition.
Decreased food intake, less fluid consumption, and taking two meals, were found to contribute to malnutrition in those patients. Moreover, age, marital status, economic dependency, type of family, and education were associated with nutritional status in the elderly, with increased age, unmarried status, and living in extended families being significant factors contributing to malnutrition.10
Even though many of the community-dwelling adults suffer from comorbid conditions and have a risk for nutritional problems, much attention has not been given to an assessment of nutritional status among older adults in the community. This study is an attempt to assess the nutritional status of older adults in the community and to identify the common nutrition problems present among older adults in the community.
Materials and Methods
The study was approved as a part of the community project for fulfilment of the requirement of completion of the academic degree course in the Bachelor of Science in Nursing Program. The study used a quantitative approach with convenience sampling. The participants of the study were adults above 50 years residing in ward 11, Athirampuzha panchayat, Kottayam. The data collection was carried out from 05/09/2024 to 12/09/2024. Participants were included if they were above 50 years, and if they are willing to participate in the study. They were excluded if they were suffering from any acute illness, post-surgery, or any other conditions in which the participants may have already existing nutritional problems.The ethical permission for conducting the survey was obtained from the authorities. The data collection was carried out along with a large community survey conducted in this area.
Tools for data collection
The tool of data collection was developed after an extensive review of literature and deriving suggestions from subject experts in the field. The investigators incorporated the nutritional assessment questionnaire with this large community survey questionnaire.
The following tools were used in data collection:
Sociodemographic tool: Demographic data were collected using a structured questionnaire which consisted of information like age, gender, type of family, marital status, educational qualification, employment status, type of employment, and monthly income.
Structured questionnaire for Anthropometric measurement: This part consisted of questions related to anthropometric measurements of older adults. There questions were related to height, weight, BMI and waist circumference. Based on the BMI of each adult they are categorized into underweight, normal, overweight as per WHO guidelines.
Nutritional risk factor assessment questionnaire: This semi-structured questionnaire consisted of 20 questions including items related to food habits, patterns, intake of nutritious food, sources, and other existing risk factors or co-morbidities. The questions were developed by a thorough literature review of articles published in elderly or older adult groups with a specific mention about nutrition, and its related factors. The tools were validated by subject experts who are the faculty having clinical exposure to the geriatric population
Data collection process
After obtaining formal permission from the authorities, the data collection was carried out during the month of September, from 05/09/2024 to 12/09/2022. All the participants were recruited after explaining the purpose of the study and taking informed consent from them. Samples who fulfilled inclusion criteria were selected by convenience sampling technique. A structured questionnaire was used to collect data regarding the nutritional status and prevalence of nutritional problem among older adults. Around 15-20 minutes was taken by the samples to answer the structured questionnaire.
Results
Findings related to socio-demographic characteristics of the participants
The sociodemographic characteristics of the participants are shown in (Table 1 )
A total of 50 older adults participated in the survey. The majority of the participants (n = 28, 56%) belonged to the age group of 50-55 years, males (n= 26, 52%), with high school education (n =17, 34%), married (n =48, 96%), and belonged to nuclear families (n = 33, 66%). The employment status showed that a majority of them were unemployed (n= 38, 76%). Those who were employed mostly belonged to private sector (n=20, 40%) with a monthly income less than Rs. 10,000 (Table 1).
Table 1
Socio-demographic characteristics of the participants
Findings related to anthropometric measurements of older adults
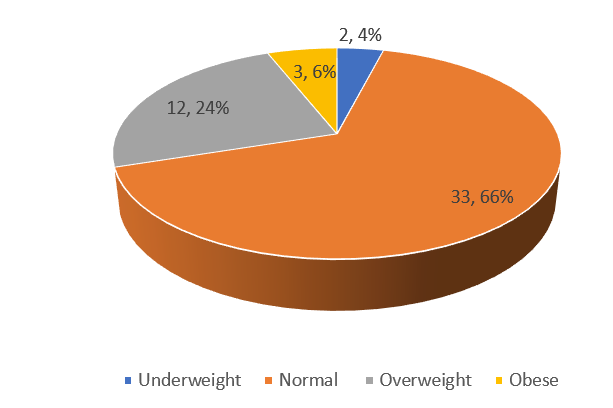
The present study shows that 33 participants (66.0%) had a normal BMI, 12 participants (24.0%) had a high BMI which indicated overweight, 3 of them (6%) were obese and 2 participants (4.0%) had a low BMI which indicates underweight (Figure 1). The waist circumference of 26% of the participants were above normal.
Findings related to nutritional assessment of older adults
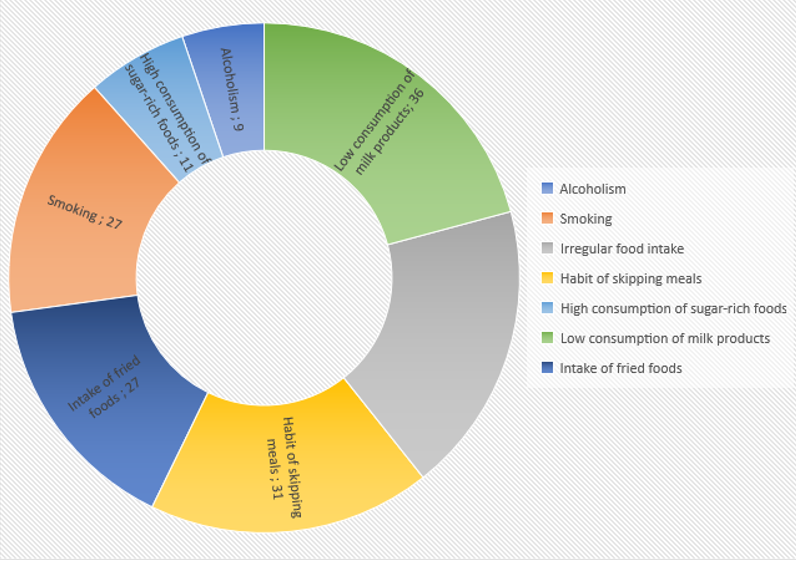
The present study revealed that a majority of older adults (n= 46, 92%) were non-vegetarians, 27 participants (54%) had a preference for fried foods, and about 32 participants (64%) had a habit of eating fast food or from outside the home. A majority of the participants (n = 32, 64%) had an irregular food intake, and 31 of them had the habit of skipping meals (62%.). Nearly 36 participants (72%) had a low consumption of milk or milk products. Half of them (50%) consumes green leafy vegetables once in a while, whereas 17 of them include fish most often in their diet. Alcoholism and smoking were reported among 9 and 27 of the participants (18% and 54% respectively). Most of them (n = 45, 90%) do not include multivitamins in their diet. Moreover, 22% of them (n=11) consumed sugar-rich foods at a higher rate (Figure 2).
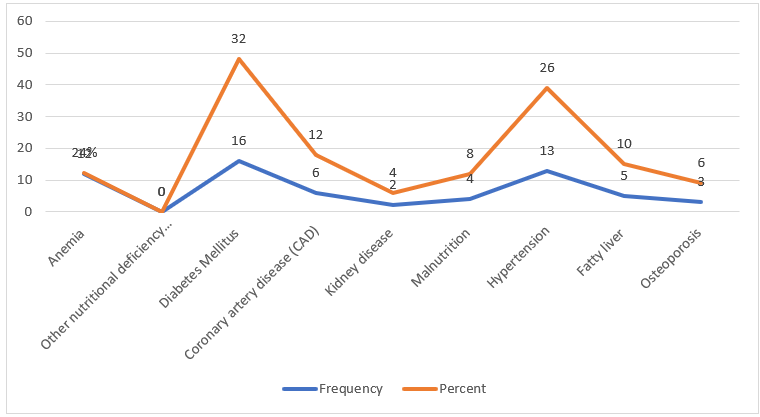
The presence of clinical and nutritional risk states is given in Figure 3. A majority of them had diabetes, followed by hypertension, coronary artery disease, and fatty liver.
Discussion
The present study was done to assess the nutritional status and problems of older adults in a selected rural area of Kerala. Many of the present study results supported other studies carried out in different parts of the country and world, with consistent results, especially with regard to the demographic risk factors influencing nutritional status among older adults. The findings of the present study are discussed with reference to the related literature and in relation with other supportive studies carried out by researchers in different settings.
The present study results showed that the majority of the participants were males and belonged to 50-55 years, having high school education, married, unemployed, with a low income and belonging to nuclear families. Whereas in a recent study carried out by Abraham in one of the districts in Kerala, 2 the majority of the participants who were at risk of malnutrition had up to middle class education, females, and were above 80 years, unemployed, and belonged to rural area, with a status of either widowed or separated. The same study also reported that education status, occupational status, place of residence, marital status, and monthly family income were significantly associated with the nutritional status.
The present study shows that 36 participants (72.0%) have normal BMI, 12 participants (24.0%) have a high BMI which indicates overweight, and 2 participants (4.0%) have a low BMI which indicates underweight. Lifestyle factors such as busy schedules and quick meal management disrupts hunger regulation and promotes overeating, and drives ultra-processed food consumption. One study carried out among Mexican-American had found that cultural factors can influence weight gain and obesity.11 Few other studies have reported that type 2 diabetes mellitus is related to an increase in BMI and excess weight gain in 90% of cases, and is one of the most common comorbidities.11, 12, 13, 14 Our present study also found that about 32% of the participants reported with diabetes mellitus. But a study conducted in Pathanamthitta district of Kerala to assess the nutritional status of people above 60 years of age, hypertension was reported as the commonest comorbidity among the study population.2
Nearly 62% of the participants in the present study had reported that they skip their break-fast. One of the prospective studies conducted in Rhode Island among a large sample of subjects during their transition in adulthood, reported that fast food consumption, decreases in breakfast consumption predicted an increase in BMI, along with the dietary behaviors. 15
The present study reported that 4% of the subjects were below the normal weight. This was in contrast to a study result of Abraham et al.,2 where 11.6% of the study participants were malnourished. The same study also reported that one-eighth of their participants were obese and another one-fourth were overweight. Moreover, education, place of residence, marital status, and family income significantly influenced nutrition status in elderly. A study done by Ghimire S., Baral B, and Callahan K on nutritional assessment of community dwelling older adults in rural Nepal had reported that 24% of the participants were malnourished, which was higher among females than males. Also, those with better literacy had a better nutritional health than their counterparts.16 In an urban-based study carried out in Coimbatore, Tamil Nadu district, India among 190 elderly to assess the prevalence and correlates of malnutrition showed that 19.7% (n = 37) were malnourished and 47 (24.73% ) were at risk of malnutrition. 17
Lifestyle related factors were stronger predictors of the nutritional status among community dwellers. In the current study, a majority of the participants had an irregular food intake with a habit of skipping meals, and a low consumption of milk and milk products. They also had a preference to fried foods and a habit of eating from outside. Moreover, habits of alcoholism and smoking were present among the males. In a study carried out in India by18 Sendhil, et al.,18 consumption of protein intake was consistent among rural and urban areas, whereas fat consumption varied, and the nutrients consumption level was lower in majority of states. In the same study, it was reported that nutrient intake in rural India is influenced positively by per capita expenditure on food items, household size and literacy rate and negatively by poverty rate. In another population-based longitudinal study conducted in India,19 it was observed that the prevalence of underweight is almost equal among male and female older adults aged from 45-59 years, whereas a higher burden of overweight (26%) and obesity (11%) were seen among females compared to males. Also, males above 60 years and above carried a higher burden of underweight (28%) than all other sub-groups.19 In the same study, it was reported that widowed and other non-married individuals, elderly who lives with spouse and/ or others, individuals with low educational status, elderly living with a small household size, those from poor socioeconomic background etc. are more likely to be underweight than others. Whereas, a cross-sectional study carried out in Tamil Nadu reported no significant association observed between smoking, current alcohol consumption, higher medication use, and higher comorbidity, with malnutrition, but gender and single/widowed/divorced status were predictors of malnutrition.17 It has to be understood that in a community setting, the social environment in which the older adults live, plays a crucial role in changing the dietary patterns. The accessibility and availability of foods, finance, and mobility restrictions have become major challenges when it comes to nutritional habits among the elderly which require a lot of family support. The changes in demographic factors in which most of the children in the households leave their parents for jobs make them live in isolation and neglect their health or nutritional status.19
To conclude, various research studies had demonstrated that a striking influence is present between the demographic characteristics, anthropometric Measurements and Nutritional Assessment of Older Adults. These findings provide insight on the nutritional pattern of older adults and the various factors influencing the nutritional pattern and risk factors for nutritional problems.
Strength and limitations of the study
The study provides useful information about the trends in the nutritional status of the population in Kerala. Many studies have been conducted among Indians, but most of them have focused on BMI and other factors influencing BMI, and the interrelationships between sociodemographic factors and nutritional status were not studied much. This study was a small attempt to investigate the nutritional risk factors and the status of nutrition among the elderly. The major limitation of this study was that we used convenience sampling, which may limit the representation of the population of interest being studied. The questions were derived from a short survey conducted in the community, which delimited the study results. Since the study was a descriptive survey, associations with sociodemographic variables could not be calculated. The samples were people who were present in the houses during the survey, and thus may not be representative of a large population, to be carefully considered for generalization of the study results. Future studies can be conducted with a large sample of the older population and can be directed to yield nutritional status results in both males and females separately. A more detailed study can be undertaken to examine the demographic factors and other contributing factors affecting nutrition status of the older adults and can examine the association of various factors influencing the nutrition status of the older adults in the community.
Conclusion
The present study was done to assess the nutritional pattern and the nutritional risk factors among older adults in a selected rural are of Kottayam. Many of them had lower educational background and were unemployed, and had food outside their homes, and engaged in unhealthy habits. This could be attributed to the pattern of older adults’ behavior in the community, by not eating food from home, but rather skip their meals or had irregular eating patterns which could result in many of the nutritional problems. Further studies are required to explore the nutritional status further, by conducting the same study in a larger sample of population and looking at their dietary habits and physical activity, and other health-seeking behaviors.