Introduction
According to the International Diabetes Federation (IDF), approximately 537 million individuals globally are affected with diabetes, constituting roughly 10.5% of the world's populace aged from 20 years to 79 years. 1 According to the World Health Organization, noncommunicable diseases claimed about 74% of global deaths in 2019, notably, diabetes emerged as a significant contributor, accounting for 1.6 million fatalities, securing its position as the ninth leading cause of death worldwide. 2 Diabetes is characterized by persistently high blood glucose levels due to inadequate insulin production or when the body fails to utilize the insulin when it is produced. Diabetes affects individuals of all ages, genders, and geographic locations, making it one of the most prevalent global causes of mortality and morbidity. Hereditary and environmental factors contribute to the etiopathogenesis of type 2 diabetes, which makes up over 90% of all instances. The most common types of DM are type 1 and 2; both have recognized diagnostic criteria and are projected to have an increase to 12.8% by 2045. 2
The world statistics indicate that diabetes was responsible for 6.7 million deaths in 2021, which is one death in every five seconds. 3 Significant risk factors towards pre-diabetes and diabetes in the population include impaired glucose tolerance (IGT), decreasing levels of physical activity, an increasing trend towards overweight and obesity, eating junk or processed foods, apart from the aging population, and a shift towards urbanization. 4, 5 Kerala is the diabetes capital of India with a prevalence of diabetes as high as 20% - double the national average of 8%. 2 Diabetes can be reversed, or controlled, if the necessary steps are taken by the individuals to modify their lifestyle and adopt a healthy lifestyle and dietary habit. 2
Evidence from a cohort study in Central Kerala indicated that people living in the rural community of Kerala were largely observed to have sedentary lifestyle habits, and impaired glucose levels, with family history and age emerging as significant risk factors for the high prevalence of diabetes mellitus in the community. 6 Thus, the present study assessed the prevalence and risk factors of diabetes mellitus among adults in a selected rural community of Kerala.
Materials and Methods
The study was conducted as a part of the community survey, a partial fulfillment of the requirement of completion of the community health clinical practical requirement of fourth year B.Sc. Nursing program. The study used a quantitative approach, with a descriptive, cross-sectional survey design. The participants were 824 adults, aged above 21 years, and residing at two selected wards of Athirampuzha panchayat, Kottayam district, Kerala. The participants were recruited using a convenience sampling method, after getting permission from the authorities. Convenient sampling was chosen in this study because it was conducted within a strict time frame for the students to suit their curriculum requirement as a part of performing community survey and was feasible.
The data was collected using a structured questionnaire with three parts: a socio-demographic part, lifestyle-related factors, and a specific part for collecting diabetes-related information. Ethical permission was obtained from the concerned authorities for performing data collection as a part of community survey which is a university requirement of the students .Data collection was carried out from July 2024 to September 2024.
Tools for data collection
The tool was developed after an extensive review of literature, consultation with experts, and preparation of a blueprint. From this, the investigators developed a structured questionnaire to assess the prevalence and risk factors among people with diabetes mellitus in a selected rural community.
Section–A: Sociodemographic characteristics of the people: This section consisted of information about age, sex, type of employment, nature of the job, marital status, religion, occupational status, and type of family.
Section–B: Lifestyle-related factors: This section consists of information about the BMI, type of food and food patterns, physical activity, BMI, and habits of the selected community in Kottayam.
Section–C: Diabetes-related information: Participants’ information related to familial risk factors, duration of diabetes, type of treatment taken, and comorbid conditions.
Data collection and analysis
After obtaining formal permission from the authorities, the data collection was carried out as a part of a larger community assessment survey. The participant's information was extracted from the information obtained through the survey and analyzed using descriptive statistics.
Results
Socio-demographic and clinical characteristics of the participants.
The details of sociodemographic characteristics of the participants are given in Table 1.
A total of 824 people participated in the survey, and 131 were reported to have diabetes mellitus (15.90%). A majority of them were above 50 years (n= 107, 81.68%), females (n =69, 52.67%), homemakers (n =72,54.96%), unemployed (n =76, 58.02%), and belonged to nuclear families (n=81, 61.83%).
Regarding the clinical characteristics, a majority of them were diagnosed with diabetes within the past 5-10 years (n= 47, 35.88%), using oral hypoglycemic agents (n=107,81.68%). Among 131 diabetic patients, 42 of them had familial risk factors (32.06%). About the comorbid conditions presented along with diabetes, 55 of them (41.98%) had hypertension.
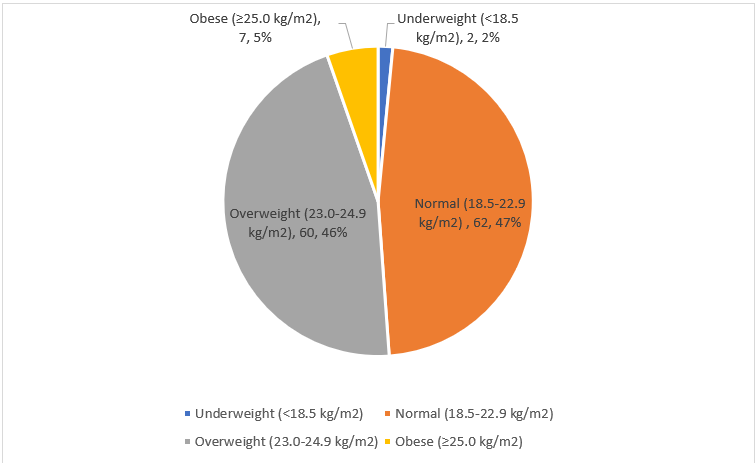
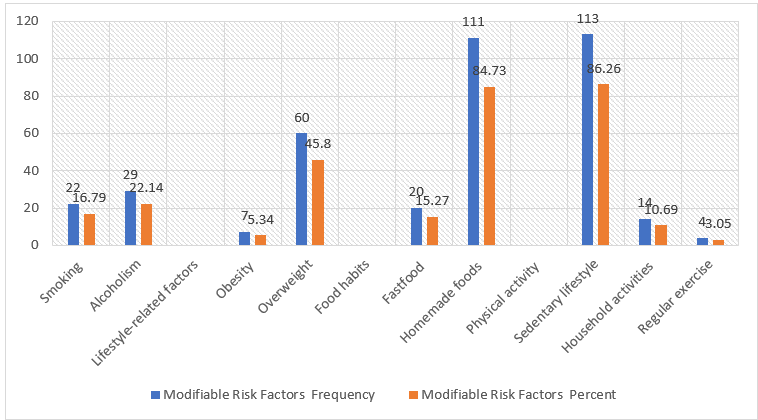
The lifestyle risk factors of the participants are as follows: a majority of them were overweight, with a BMI of 25.0-29.9 (n =60, 45.8%), and about 5.34% of them (n=7) were obese. Most of them were following sedentary lifestyle habits (n 113, 85.93%), and were Nearly 15.27% of them were eating fast foods (n=20), whereas 84.73% of them (n=111) were taking homemade foods. (Figure 1, Figure 2)
Table 1
Sociodemographic and clinical characteristics of the participants N=131
Discussion
The study focused on assessing the risk factors and the prevalence of diabetes mellitus among a small rural community in Kerala. The study results demonstrated that females were more affected by diabetes mellitus, and the prevalence of diabetes mellitus in the community is 15.90%. This is slightly lower than the reported rate of diabetes in Kerala, which is 19.4 %. 7However, similar to our study results, a cohort study conducted in Kerala reported that females were largely affected by diabetes mellitus. A recent ICMR study in fifteen states found a mean prevalence of 7.3 percent. In a study conducted in Bangladesh, 36.9% were treated and 14.2% were reported with controlled diabetes. 7 Though diabetes was more common in urban areas and in higher socioeconomic groups, it was seen that in seven states, rural prevalence was seen which was associated with a lower economic group. 6 A prospective study estimates that the cumulative incidence of type two DM in Kerala is 21.9% and the incidence of prediabetes is 36.7%. Nearly 60% of the participants who had impaired plasma glucose at baseline converted to type two diabetes mellitus at present, showing an epidemic trend for type 2 diabetes mellitus in Kerala. The findings of this study provide conclusive evidence that the incidence of type 2 DM and prediabetes is increasing rapidly in developing countries. 8
In the current study, diabetes is found to be higher in nuclear families, those who are unemployed, and homemakers. Moreover, family risk factors were present among 32.06% of them. Similar to these results, a study conducted in Kerala showed that a family history of diabetes was present among 28.2% of the participants, which had emerged as a significant risk factor for diabetes. 6, 9 In contrast to the current study findings, a study conducted in Bangladesh demonstrated that the occurrence of diabetes mellitus was 62% higher for higher-educated participants, and 42% higher for those who came from rich families. 10
Also, 16.79% had modifiable unhealthy habits like smoking, and 22.14 of them reported to have alcoholism. Similarly, a majority of the participants were following a sedentary lifestyle (86.26%, n =113). This was in contrast to the study results obtained in Kerala, were 21.8% of the participants reported have regular physical activity. 5 Whereas a study carried out among the elderly in China had reported BMI, central obesity, education level, marital status, physical activity, alcohol consumption, and age were factors associated with diabetes prevalence. 11
Thus, in this survey, a sedentary lifestyle had emerged as the significant risk factor in diabetes, along with family history, and gender. Moreover, hypertension was found to be the leading comorbid condition affected by diabetic individuals. These were similar to the study results reported in two prevalence studies conducted in Bangladesh and also in China.
10, 12, 13 Also, in a prevalence study conducted in an urban settlement in Kerala, it was found that diabetes is associated with advancing age, body mass index above 24.99, sedentary habits, hypertension, smoking, and serum total cholesterol above 239, and serum triglycerides above 149. 14 The current study also reported a higher prevalence of diabetes with BMI greater than 24.99, sedentary lifestyle pattern, hypertension, and smoking. Overweight/obesity and central obesity were emerged as the most important modifiable risk factors for developing T2DM in Kerala. 6 Age, marital status, hypertension, obesity, and family history of diabetes mellitus were significant risk factors for diabetes mellitus in a study carried out in Panjab, India. 15 In another study carried out in an urban settlement in India, a low prevalence of diabetes, i.e., 9.88%, with an increased prevalence with advancing age, as well as male gender, obesity, waist circumference, and an increase in waist-hip-ratio was reported. 16
This study provides knowledge of the prevalence of diabetes in a small rural area of Kottayam. The main limitations of the study were the use of non-probability sampling technique,i.e., convenience sampling, and therefore, may not be fully representative of the population being studied. Also, the study was performed in participants residing a small rural area of Kottayam District who may be culturally different from people belonging to other parts of the state. We also could not perform a laboratory analysis of cholesterol and other biochemical results, which would have contributed to a more reliable finding in this study.
Conclusion
Our study gives an insight into the depth of the diabetes prevalence in the community, which warrants early detection, follow up of the compliance to treatment in those with diabetes and a change in the lifestyle pattern of the residents. Further studies can be conducted with a larger sample and include more participants from different localities. In addition, those studies can perform a data collection with more explicit data sampling methods using probability sampling technique, or by stratified random sampling to get a gender-based difference in diabetes mellitus as well as by using biochemical markers to identify risk factors in community.