- Visibility 25 Views
- Downloads 6 Downloads
- DOI 10.18231/j.agems.2022.011
-
CrossMark

Risk factors and health-seeking behaviours in non-communicable diseases among a community sample of women
- Author Details:
-
 Bindu John *
Bindu John *
-
Usha Marath
-
Aleena Babu
-
Anit Jiji
-
Anitta Babu
-
Anu Joshy
-
Athira PR
Introduction
The global burden of non-communicable diseases (NCDs) had increased tremendously, causing increased morbidity, mortality and disability among population, which is impeding the standards of health, quality of life and productivity among people at every age as well as affecting the socioeconomic development of the country.[1] NCDs accounts for about 70% of all global deaths, i.e., about 38 million deaths annually.[2] In 2019, it accounted for 1.62 billion Disability Adjusted Life Years (DALYs), representing 63.8% of total DALYs.[3] NCDs are no longer limited as a leading cause of death in high income countries, and the recent statistics by the World Health Organization (WHO) reports that it is a major cause of death in most low-income and middle-income countries, accounting for about 80% of premature deaths, i.e., under 70 years of age.[4], [5], [6] By 2030, NCDs are predicted to cause a collective loss of $47 trillion which can affect the young population’s productivity.[7]
Cardiovascular diseases remain as a major NCD affecting public health, and resulting in mortality among people, accounting for about 17 million deaths approximately in the World,[8] and 23% and 30% of the total mortality in rural and urban population, respectively, in India.[9] Rapid urbanization, industrialization, and globalization resulting in economic transition which in turn influences the health risk behaviour of people has been identified as a major trend influencing the risk of burden of disease among the population.[9] Increased burden of obesity, hypertension, diabetes and dyslipidaemia had risen the risk factors and subsequent development of CVDs in the country.[9]
Evidence from a recent research study conducted in Himachal Pradesh, India reports a 19.7% and 6.9% of prevalence of hypertension and diabetes respectively in the population, which had increased significantly with increasing age.[9] This study also reports that while hypertension had been reported in a significantly higher level in men (22.4% vs. 17.5%), diabetes was more prevalent among women (7.6% vs. 6.0%). Moreover, overweight and obesity was also reported at a significantly higher rate among women, compared to that in men. However, research indicates that tobacco use, physical inactivity, unhealthy diets, and harmful use of alcohol can be attributed as common risk factors for the four major NCDs (cardiovascular diseases, diabetes, cancer and chronic respiratory disease),[9], [10] along with age.
Health seeking behaviours has been described as a sequence of events undertaken by the individuals as remedial to perceived ill-health,[11] and can be influenced by various elements, including socio-demographic, economic factors, as well as the accessibility and affordability of medical services.[12] Health-seeking behaviours in the population can be targeted at modifiable risk factors, such as high blood pressure, smoking, diabetes mellitus, physical inactivity, obesity and high levels of blood cholesterol, in order to improve the health status of the population.[4], [9], [13] Health-seeking behaviour is one of the important determinants of women’s health, which can be influenced by their individual knowledge, disease perception, socio demographic factors, and the availability and accessibility of health services.[14], [15] Health-seeking behaviour of women is an important factor in preventing NCDs, as it can -influence the health of the family through influencing lifestyle and related changes.[16]
Therefore, identifying health-seeking behaviours and risk factors among women is important to determine factors contributing to NCDs and to lessen the incidence of NCDs in the community.
Thus, this study aims to assess the risk factors and health-seeking behaviours in non-communicable diseases among a community sample of women.
Materials and Methods
The study was conducted as a part of the research project, as partial fulfillment of the requirement of completion of the academic degree course in the Bachelor of Science in Nursing Program. The study used a quantitative approach, using a descriptive, cross-sectional survey design. The study was conducted in Kerala, India. The participants were 100 adult women, aged between 35 and 55 years, and having diagnosed with hypertension, diabetes, or dyslipidaemia. The data collection was carried out in October 2022.
The study participants were recruited using a convenience sampling method, after getting permission to perform the study from the local authorities. They were included if they were adult women belonging to the age group of 35 – 55 years, can read and write Malayalam language, if they had been diagnosed with or on treatment for NCDs such as diabetes mellitus, hypertension, and/ or dyslipidaemia, and if they were willing to participate in the study. Participants were excluded if they were deaf and blind, mentally challenged, and a transgender. A written consent was taken from all the participants, who agreed to participate in the study.
Tools of data collection
The following tools were used in data collection
Demographic-clinical questionnaire: This semi-structured questionnaire consisted of a few demographic items such as age, education, marital status, religion, occupation, type of employment, income, type of family, and clinical parameters such as height and weight, type of NCD, and duration of illness.
Risk factor assessment questionnaire for NCDs: Developed and adopted by the researchers, this 20-item, semi-structured questionnaire was designed to assess the risk factors present among women. The content validity of the questionnaire assessed through a content validity index (CVI) was 0.96 and the reliability established through a test-retest method was found to be 0.96.
Health-seeking Behaviour Assessment Rating Scale: This 21-item rating scale was developed and adopted by the researchers, and was designed to assess the health-seeking behaviours among women. The items were scored on a 5-point rating scale (5= Always, 4= Often, 3= Sometimes, 2= Rarely, and 1= Never). The total items summed up gave a total score range of 21-105. The scores were categorized as excellent (ranging from 89-105); Good (ranging from 72-88); Average (ranging from 55- 71); below average (scores ranging from 38-54); and poor (scores ranging from 21-37). The scale demonstrated a content validity index of 0.98, and a test -retest reliability of 0.8.
Data collection process
After obtaining formal permission from the authorities, the data collection was carried out during the month of October, from 19/10/2022 to 27/10/2022. All the participants were recruited after explaining the purpose of the study and the study procedure. The participants who gave informed consent were approached and the questionnaires and rating scale were distributed. Completed questionnaires were collected 30 minutes after their administration.
Results
Demographic characteristics of the participants
The details of sample characteristics are given in [Table 1].
A total of 100 adult women aged between 35-55 years participated in the survey. A majority of them (39 percent) were aged between 51-55 years, were having primary education (30 percent), married (92 percent), unemployed (71 percent), and home makers (57 percent). A large proportion of them were Hindus (59 percent) and belonged to low-income levels (57 percent). All of them belonged to nuclear families (100 percent).
The clinical parameters are presented in [Table 2]. A majority of the participants (47 percent) had been diagnosed with diabetes mellitus, 45 percent of them had hypertension and 28 percent were having dyslipidaemia. Most of them had developed the disease in less than 5 years (50 percent), and had a normal body mass index between 18.5 – 24.9 Kg/m2 (63 percent).
|
Demographic Variables |
Frequency (Percent, N= 100) |
|
Age (in Years) |
|
|
35-40 |
9 |
|
41-45 |
22 |
|
46-50 |
30 |
|
51-55 |
39 |
|
Education |
|
|
No formal Education |
4 |
|
Primary School Education |
30 |
|
Secondary School Education |
29 |
|
Pre-degree/ Plus two |
19 |
|
Degree/Post-graduation |
18 |
|
Marital Status |
|
|
Married |
92 |
|
Unmarried |
1 |
|
Widow |
7 |
|
Types of Employment |
|
|
Government Sector |
9 |
|
Private Sector |
21 |
|
Retired |
12 |
|
Home Maker |
57 |
|
Own Business |
1 |
|
Nature of Job |
|
|
Household Work |
71` |
|
Manual labour |
11 |
|
Professional |
7 |
|
Office Job |
10 |
|
Technical Field |
1 |
|
Religion |
|
|
Hindu |
59 |
|
Christian |
36 |
|
Muslim |
5 |
|
Income |
|
|
≤ Rs. 10,000/- |
57 |
|
Rs. 10,000-≤Rs. 50,000 |
41 |
|
Rs. 50,000- ≤ 1,00,000 |
2 |
|
Variables |
Frequency (Percent, N= 100) |
|
Non-Communicable Diseases Present |
|
|
Diabetes Mellitus |
47 |
|
Hypertension |
45 |
|
Dyslipidaemia |
28 |
|
Duration of Illness |
|
|
≤ 5 Years |
50 |
|
5-≤10 Years |
36 |
|
10- -≤15 Years |
9 |
|
≥ 15 Years |
5 |
|
Body Mass Index (Kg/m2) and Category |
|
|
≤ 18.5 (Underweight) |
2 |
|
18.5-≤ 24.9 (Normal Weight) |
63 |
|
25-≤ 29.9 (Over Weight) |
25 |
|
≥ 30 (Obese) |
10 |
|
Pattern of Activity/ Exercise |
Frequency (Percent, N= 100) |
|
Perform Regular Exercise |
|
|
Yes |
68 |
|
No |
32 |
|
Usage of Stairs on a Regular Basis |
|
|
Yes |
59 |
|
No |
41 |
|
Type of Exercise Performed |
|
|
Walking |
52 |
|
Workout in Gym |
8 |
|
Household Activities |
4 |
|
Workout using Internet/ Web-based |
6 |
|
Frequency of Performing Exercises |
|
|
Daily |
55 |
|
Weekly |
3 |
|
Once in a While |
6 |
|
No Fixed Pattern |
4 |
Risk factors of NCDs present among women
Among 100 participants, 46 of them had a family history of NCDs whereas 54 of them did not have any family history of NCDs.
The activity and exercise pattern of the participants is illustrated in[Table 3]. A majority of the participants were using stairs regularly, 68 of them performed regular exercises, and 55 of them performed the exercises on a daily basis. Walking was the most common type of exercise method adopted by majority of the participants (52 percent).
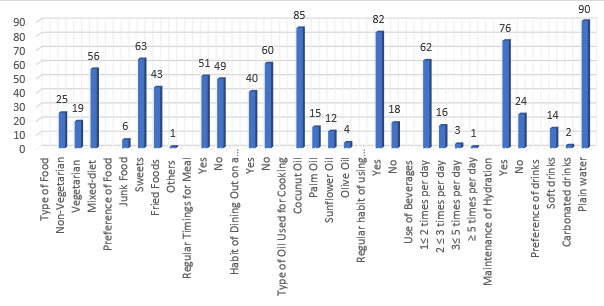
With regard to the dietary pattern, a majority of the participants (56 percent) were using a mixed diet, 25 percent were non-vegetarian and the remaining 19 percent were vegetarians. While asked about the preference of the food, 63 percent of them preferred sweets, and 43 percent preferred fried food. Use of junk foods and other types of food were comparatively less and were 6% and 1% respectively. A majority of them (51 percent) followed regular timings of meal and only 49 did not have any regular timings. More than half of the participants (60 percent) did not have any habit of dining out regularly, and 40 percent stated that they had the habit of dining out on a regular basis.
When asked about the cooking practices, 85 percent of the participants used coconut oil for cooking, 15 percent used palm oil, 12 percent used sunflower oil and 4 percent used olive oil.
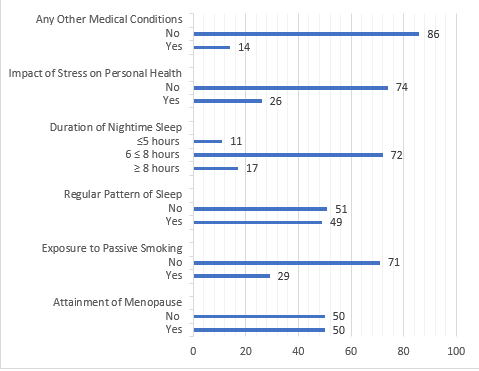
The details about the food and hydration status of women are shown in [Figure 1], and the other lifestyle-related risk factors present among the women are demonstrated in [Figure 2].
Health-seeking behaviours present among women
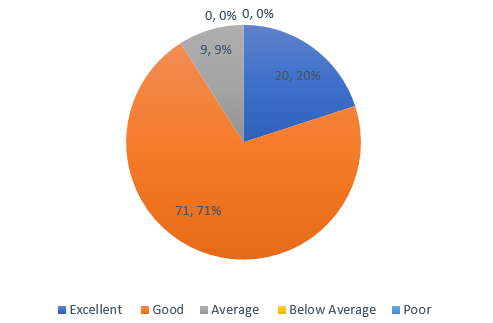
The health seeking behaviours among women is depicted in [Figure 3]. As illustrated in [Figure 3], 71 women had good health-seeking behaviours and 20 had shown excellent health-seeking behaviours. Average health-seeking behaviours were shown by 9 of them.
The study results demonstrated that a majority of the participants followed good health-seeking behaviours with regard to taking medicines prescribed by the doctor as a part of their treatment regime, performing regular exercises, utilizing NCD clinics in the health centres, consulting physician when there is a health problem, and following vaccination schedule. Nearly half of the participants practiced good health seeking behaviours with regard to engaging in activities to relax the mind, and following dietary modifications. A lesser number of participants constantly engaged in leisure time activities during their free times, and only a few participants practiced meditation, yoga or naturopathy, and following home remedies. However, a very few participants practiced self-medication, and ignored deviations in their health conditions, and demonstrated a loss of interest in practicing health-seeking behaviours such as eating healthy food, doing exercise, and not following therapeutic instructions given by doctor.
Discussion
The study results suggests that the reported hypertension in our participants were higher than it was reported in a study conducted in Vellore, Tamil Nadu, whereas diabetes is slightly less than it was reported in the same study,[17] but is higher than the reported figure in a study conducted in Kerala.[18] A rural-urban difference in high blood pressure was noted among females in a study conducted by Bhagyalaxmi (2013),[16] which was between 20-40% and 12-17 % in urban and rural adults, respectively.
The genetic risk factors in the present study were much less than it was reported in a previous study conducted by Saboo in 2021,[19] where 60% of the participants from all age groups reported to have a positive family history of NCDs. A positive family history is found to be a significant predictor for the development of NCDs, and reported to have 1.23 times more higher odds of suffering from NCDs.[20] Data reported from a research study collected from secondary data sources had reported that hypertension is one of the leading risk factors in the development of NCDs, which is showing an increased trend with urbanization, increased consumption of poultry and meat among the population.[18]
Twenty five percent of our study participants were overweight and 10 percent were obese, whereas 32.4% of the participants were reported to be obese, in a study conducted by Thomas (2020).[18] Similar to the present study results, obesity was reported among 29.9% of participants in Manipur.[20] In a study conducted in Gujarat, a high prevalence of overweight and obesity was observed both in men and women in all age-groups.[15]
A majority of the study participants were performing regular exercises, in contrast to a study where urban females had been reported to have low physical activity.[17] Sedentary lifestyle was reported among 45% of the participants and cited as a contributing factor for the development of diabetes in a large cohort study conducted among 22,921 participants from 623 sites in India.[19]
Similar to the study conducted by Poftte (2021),[20] the participants in the current study were also were consuming less junk foods, which is high in salt and dietary fat.
In the current study, the participants demonstrated good health seeking behaviours, especially with regard to their treatment regime and follow up. Similar study results have been reported by a study conducted in Kenya,[21] where females sought significantly qualified care for chronic NCDs. The same study had also reported an association of formal employment and socioeconomic predictors like higher education, marital status and having a health insurance as important predictors for health-seeking behaviours. The current study did not explore the association of socioeconomic factors for health-seeking behavioural practices.
Strengths and limitations of the study
The study highlights a major morbidity pattern and the current existing trend in the disease pattern of the population in the country. Much studies have not been conducted in this area, especially with regard to the health-seeking behaviours in women, even though risk factors have been explored in some studies in both genders. Thus, this study can be considered as a small attempt to investigate the risk factors and the health-seeking behaviours in women. The major limitation of this study was that we used a convenience sampling technique with a small sample size, which may not be a true representation of the target population, and could not include more blocks or panchayats for the data collection. This was due to the time constraints to carry out the research on a large scale. Another limitation of this study was that we could not include working population to a large extent, who would have been suffering from NCDs, and thus could not explore whether the health-seeking behaviours of the working class is different from that of the other women who was available in the community. It could be also possible that some self-reporting/self-rating bias could be present in this study, thus the results should be used with caution while generalizing study results. In addition, the paucity of studies conducted in this field had made the comparisons difficult while discussing about the health-seeking behaviours and risk factors among women.
Conclusion
The present study assessed the risk factors and health-seeking behaviours in women residing in a selected community of Kerala, India. The results suggested that the NCD risk factors are high in women, in spite of them engaging in various health-seeking behaviours. This gives an insight into exploring other factors contributing to NCDs, such as stress in the family, exercise pattern, dietary habits, other lifestyle related factors, and the time spent on gadgets using modern technology. Apart from awareness, mobilizing and participation of the community in engaging behaviours to tackle NCDs, making community- friendly areas for physical activity without fear, providing areas for walking and exercising, can make the whole community healthy. Future studies can explore research in areas like motivating factors for performing activities and the prevailing dietary habits in young generation as well.
Source of Funding
None.
Conflict of Interest
None.
References
- . World Health Organization. Global action plan for the prevention and control of NCDs. 2020. [Google Scholar]
- DC Malta, M Naghavi. Mortality due to noncommunicable diseases in Brazil, 1990 to 2015, according to estimates from the Global Burden of Disease study. 1990. [Google Scholar]
- . Noncommunicable diseases. 2022. [Google Scholar]
- HC Kim, SM Oh. Noncommunicable Diseases: Current Status of Major Modifiable Risk Factors in Korea. J Prev Med Pub Health 2013. [Google Scholar]
- . Non Communicable Diseases. 2022. [Google Scholar]
- . World Health Organization. Global Status Report on Noncommunicable Diseases 2010. 2014. [Google Scholar]
- . World Health Organization. Saving lives, spending less: the case for investing in noncommunicable diseases. 2021. [Google Scholar]
- . World Health Organization. Global Health Estimates: Life expectancy and leading causes of death and disability. 2019. [Google Scholar]
- PC Negi, R Chauhan, V Rana, K Lal. Epidemiological study of non-communicable diseases (NCD) risk factors in tribal district of Kinnaur, HP: A cross-sectional study. Indian Heart J 2016. [Google Scholar]
- TA Gaziano, N Pagidipati. Scaling Up Chronic Disease Prevention Interventions in Lower- and Middle-Income Countries. Annu Rev Public Health 2013. [Google Scholar] [Crossref]
- P Ndarukwa, MJ Chimbari, E Sibanda. Assessment of Levels of Asthma Control among Adult Patients with Asthma at Chitungwiza Central Hospital. Allergy Asthma Clin Immunol 2020. [Google Scholar]
- B Begashaw, F Tessema, HA Gesesew. Health Care Seeking Behavior in Southwest Ethiopia | PLOS ONE. PLoS ONE 2016. [Google Scholar] [Crossref]
- M Ezzati, E Riboli. Behavioral and Dietary Risk Factors for Noncommunicable Diseases. N Engl J Med 2013. [Google Scholar]
- A Budreviciute, S Damiati, DK Sabir, K Onder, PS Goetzburg, G Plakys. Management and Prevention Strategies for Non-communicable Diseases (NCDs) and Their Risk Factors. Front Public Health 2020. [Google Scholar] [Crossref]
- A Bhagyalaxmi, T Atul, J Shikha. Prevalence of Risk Factors of Non-Communicable Diseases in a District of Gujarat. India J Health Popul Nutr 2013. [Google Scholar]
- FB Rasul, M Sarker, F Yasmin, MD Allegri. Exploring Health-Seeking Behavior for Non-Communicable Chronic Conditions in Northern Bangladesh. PLOS Glob Public Health 2022. [Google Scholar] [Crossref]
- AM Oommen, VJ Abraham, K George, VJ Jose. Prevalence of Risk Factors for Non-Communicable Diseases in Rural & Urban Tamil Nadu. Indian J Med Res 2016. [Google Scholar]
- AS Thomas. Air Pollution and Nutritional Transition as Risk Factors for Non-Communicable Diseases: The Emerging Trends in Health Scenario of Kerala, India. Plant Archives. Plant Arch 2020. [Google Scholar]
- B Saboo, S Agarwal, S Gupta, B Makkar, A Panneerselvam, AK Sahoo. REAL-World Evidence of Risk Factors and Comorbidities in YOUNG Indian Adults with Type 2 Diabetes Mellitus: A REAL YOUNG (Diabetes) Study. J Fam Med Prim Care 2021. [Google Scholar]
- M Poftte, AU Rani. Prevalence and Risk Factors of Non-Communicable Disease and Healthcare-Seeking Behaviour amongst the Adults Residing in a Selected Village. Indian J Contin Nurs Educ 2021. [Google Scholar]
- KT Wanjiku. Determinants of Health Seeking Behavior Among Households with Chronic Non-Communicable Diseases in Kenya. J Health Popul Nutr 2021. [Google Scholar]