- Visibility 28 Views
- Downloads 1 Downloads
- DOI 10.18231/j.agems.2020.003
-
CrossMark

Modulating Erectile Dysfunction
Introduction
Erectile dysfunction
Erectile dysfunction (ED) is the persistent inability to achieve or maintain an erection sufficient for satisfactory sexual performance.[1] It affects about one out of two men over the age of 50. In some, ED only happens from time to time. In others, it is a more severe problem.
Sexual dysfunction takes different forms in men.
A dysfunction can be life-long and always present, acquired, situational, or generalized, occurring despite the situation.
A man may have a sexual problem if he:
Ejaculates before he or his partner desires
Does not ejaculate, or experiences delayed ejaculation
Is unable to have an erection sufficient or impotence for pleasurable intercourse.
Feels pains during intercourse
Lacks or loses sexual desire.[2]
Male menopause or Andropause
involves a drop in testosterone production in men who are age 50 or older. It’s often affiliated with hypogonadism. Both conditions involve lowered testosterone levels and similar symptoms. Approximately 30% of men in their 50s will experience symptoms of andropause caused by low testosterone levels. As men age, not only does the body start making less testosterone, but also the levels of another hormone called sex hormone binding globulin (SHBG), which pulls usable testosterone from the blood, begins to increase.
Prevalence
The prevalence associated with ED increases with advancing age. The global prevalence of ED was 3–76.5%. ED was associated with increasing age. It is 1-10% in men who are younger than 40 years of age, 2-9% in men aged between 40 and 49, and increases to 20-40% in men aged between 60 and 69 years. Thailand reported an overall prevalence rate of 37.5% amongst men 40 to 70 years of age. The prevalence of ED is 50-100% in men older than 70 years of age[[3], [4]A].
Men from Indian subcontinent are shy of talking about ED and psychological factors play dominant part in India. Asia will continues to have the largest number of 200 million men suffering from ED, reflecting a 130% growth, which is the third fastest after Africa and South America.[3]B
Basics of Penile erection
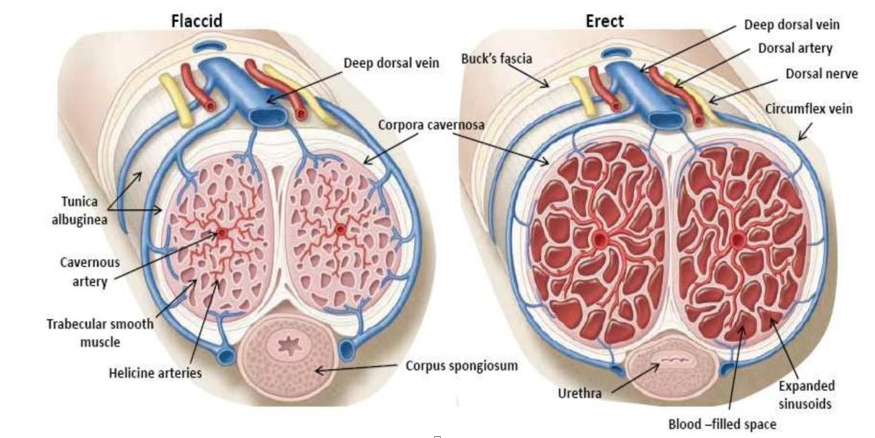
The human penile venous system is generally described as a single deep dorsal vein accompanied by a pair of dorsal arteries positioned between the tunica albuginea and Buck’s fascia for the venous drainage The corpus spongiosum (CS) is erectile tissue analogous to corpus cavernosum (CC), but with a thinner tunica albuginea. The urethra lies within the spongiosum. The innervations of the penis is both autonomic (sympathetic and parasympathetic) and somatic (sensory and motor). From the neurons in the spinal cord and peripheral ganglia, the sympathetic and parasympathetic nerves merge to form the cavernous nerves, which enter in the CC and corpus spongiosum to affect the neurovascular events during tumescence and detumescence, as shown in [Figure 1] [5], [6]
Physiology of Penile erection
The NO-sGC-cGMP pathway
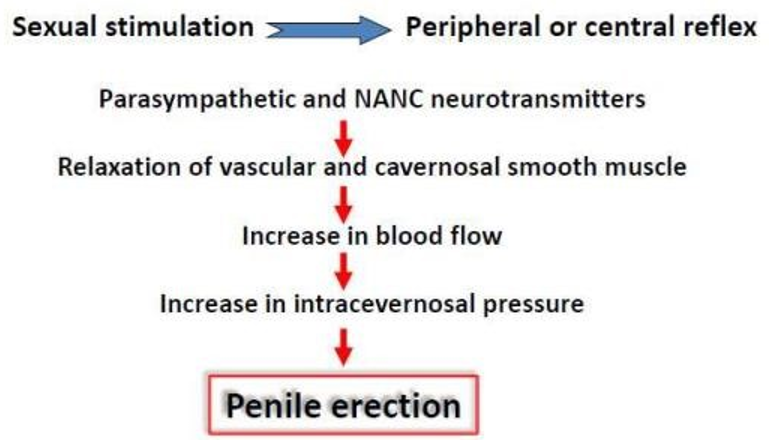
NO (Nitric Oxide) exerts its action on smooth muscle cells by activating the enzyme soluble guanylate cyclase (sGC). The activation of sGC results in an increase in intracellular cGMP concentrations. This in turn activates a number of second messenger systems, which ultimately results in smooth relaxation. The cGMP is then metabolised by the enzyme phosphodiesterase type 5 (PDE-5).Aging process reduces activity of NO, which has vasodilatory action, as shown in Figures 2 and 3.[7]
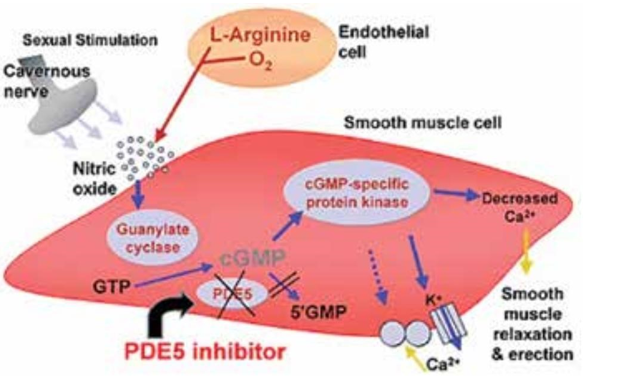
PDE5 is an enzyme found primarily in the smooth muscle of the corpus cavernosum that selectively cleaves and degrades cGMP to 5′-GMP. PDE5 inhibitors, such as Sildenafil(Viagra) , are similar in structure to cGMP; they competitively bind to PDE5 and inhibit cGMP hydrolysis, thus enhancing the effects of NO.
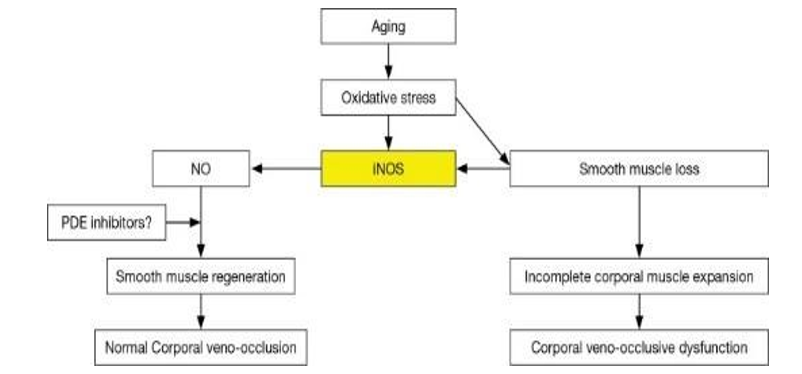
Aging leads to oxidative stress and subsequent decrease of NO which causes vasodilatation and erection of penile system, as depicted below in [8] [Figure 4]
Causes of Erectile Dysfunction: This is represented in [Figure 5]
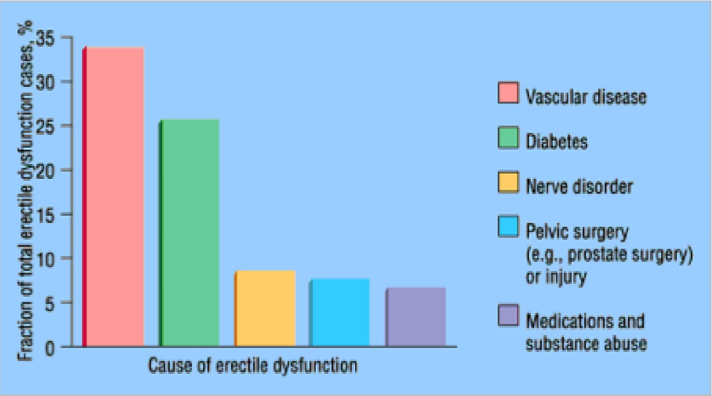
Psychological causes (e.g. depression, anxiety and stress involving the workplace) used to be considered some time ago as the most common reason for ED.
Vasculogenic. The most common single cause, due to low blood inflow (e.g. large vessel atherosclerosis). The incidence of ED in atheromatous aortoiliac and peripheral vascular disease is about 50%. Hypertension is a well-established risk factor for ED, with 30% to 50% of hypertensive men being affected
Diabetes mellitus is a common cause of organic ED, up to 75% of diabetic patients accusing poor erections. It is hypothesized that cavernosal artery insufficiency, corporal venoocclusive dysfunction, and/or autonomic neuropathy are the major organic pathophysiologic mechanisms leading to persistent erectile impairment in men with diabetes mellitus.
Obese (BMI > 30 kg/m2) men have an incremental increase in the risk of ED with the relative risk ranging from 1.5 to 3.0 fold
Pelvic fractures with ruptured posterior urethra. The damage to the neurovascular bundle or to the internal pudendal or common penile artery at the time of injury is predominantly responsible for most of the ED, Prostate surgery can trigger ED, particularly in the first year after surgery. However, sexual function improves over time for most men.
| Antihypertensive drugs | Antiarrhythmicagents | Psychotropicdrugs | GnRH agonists | Anti-androgen drugs and 5-alpha-reductase inhibitors | Recreational drugs |
| Thiazide duiretics | Digoxin | TCAs | Leuprolide | Cyclophosphamide | Marijuana |
| Β blockers | Amiodarone | SSRIs | Goserelin | flutamide | Opiates |
| Calcium-channel blockers | Disopyramide | Phenothiazines | ketoconazole | Cocaine | |
| Methyldopa | Butyrophenones | Spirinolactone | Nicotine | ||
| Reserpine | Cimetidine | Alcohol | |||
| Doxazozin | Cyproterone | ||||
| Finasteride | |||||
| Dutasride |
ED is a common side effect of selective serotonin reuptake inhibitors (SSRIs), with the incidence ranging from 20 % to 80 % depending on the medication utilized.
Diagnosis of Erectile Dysfunction
Panel investigations in ED

A few validated instruments are used in diagnosing ED, grading its severity, and assessing treatment satisfaction. Some examples of such instruments are the International Index of Erectile Function (IIEF), the Modified 5-item version of IIEF (IIEF–5), and the Erectile Dysfunction Index of Treatment Satisfaction (EDITS). The IIEF is a self-administered 15-item questionnaire consisting of five distinct domains: erectile function (total score range 1– 30), orgasmic function (total score range 0–10), sexual desire (total score range 2–10), intercourse satisfaction (total score range 0–15), and overall satisfaction (total score range 2–10). Recommendations based on biochemical investigation may consist of hormonal screening to detect hypogonadism or other underlying common diseases such as hyperprolactinemia, diabetes and dyslipidemia. Other methods that may be used are urine analysis, blood count, lipid levels, or prostate-specific antigen (PSA) concentration. There are also specialized evaluation techniques such as duplex ultrasonography, penile tumescence studies, RigiScan, test injections, audio- visual stimulation and penile brachial index measurement.[10]
Treatment options for erectile dysfunction conservative medical therapy
Role of testosterone
Both ED and low testosterone (hypogonadism) increase with age. The incidence of the latter is 40% in men aged 45 years and older. Testosterone treatment does not improve erections in men with normal testosterone levels and it does not help men with low testosterone levels if ED is their only symptom.
Androgens have always been assumed to play a major role in male erectile function with hypogonadism because:
There is a decrease in serum testosterone levels with aging and a time period when the prevalence of ED increases.
Castration usually causes a decline in sexual function.
Sexual function returns to normal in castrated (severely hypogonadal) men who undergo treatment with exogenous androgens.
Oral agents for testosterone replacement are clearly convenient and comfortable to use. Oral testosterone, however, is absorbed rapidly from the GI tract and circulates through the portal blood.
Testosterone undecanoate, is available only outside of the United States. 45 The usual dose is 120 to 240 mg/d, divided over 2 or 3 doses. The most effective of oral agents of testosterone are the 17 alkylated testosterones, such as methyltestosterone. These 17 alkylated testosterones may be administered either orally or buccally Intramuscular preparations of testosterone are effective in increasing serum testosterone levels. In men requiring testosterone replacement, testosterones enanthate and cypionate may be administered every 2 to 3 weeks to maintain normal average testosterone levels, Transdermal testosterone is currently available as a scrotal or nonscrotal patch.
Testosterone treatment can cause the body to retain too much fluid. It can also cause acne, an enlarged prostate, and enlarged breasts. Other side effects include lower fertility;
An increase in red blood cells; and an increase in sleep apnea symptoms.
Replacing testosterone in the blood is the most common treatment for men going through andropause. This treatment may provide relief from the symptoms and help improve the quality of life in many cases.
Intracavernosal injection of VEGF (vascular endothelial Growth factor) appears to restore smooth muscle integrity and improve erectile function in aged rats. Intracavernous injection of the VEGF gene may be a preferred therapy to preserve erectile function in patients in whom testosterone therapy is contraindicated.[11]
Treatment Algorithm for Erectile Dysfunction
Assessment of treatment options includes a patient-focused discussion incorporating information about risk factors and lifestyle needs. Treatment options should be tailored to individual patient and partner satisfaction, quality- of-life factors, and treatment-related safety and efficacy considerations.

First Line Therapy
Properties of oral 5 phosphodiesterase inhibitors [[12] A]
Mode of action
PDE5 is an enzyme found primarily in the smooth muscle of the corpus cavernosum that selectively cleaves and degrades cGMP to 5′-GMP. PDE5 inhibitors are similar in structure to cGMP; they competitively bind to PDE5 and inhibit cGMP hydrolysis, thus enhancing the effects of NO. PDE5 inhibitors lack a direct effect on corpus cavernosum smooth- muscle relaxation.
Pharmacodynamics
Mammalian phosphodiesterases (PDEs) comprise 11 gene families, which are distributed in different areas of the body. Each PDE family contributes to various physiological functions. Because the smooth muscle of the corpus cavernosum expresses type-5 PDEs predominantly, the specificity and selectivity of PDE5 inhibition play a crucial role in prolonging erections and in limiting adverse effects from nonspecific PDE inhibition.
Relative safety of Vardenafil (BAY 38-9456) & Avanafil(Stendra)
Less selective against PDE6, which is expressed in the retina. Patients have reported less vision-related adverse effects consistent with PDE6 inhibition, such as dose- related impairment in color discrimination (blue/green) or cyanopsia (objects appearing blue).
Relative activity
Vardenafil (Levitra) improved erections in difficult-to-treat subgroups. In diabetic patients, 72% reported improved erections. Tadalafil (Cialis) has drop-out rate due to adverse events is similar to placebo. Tadalafil, 5 mg daily, therefore provides an alternative to on-demand dosing of tadalafil for couples who prefer spontaneous rather than scheduled sexual activities.
Choice of drug
Depends on the frequency of intercourse (occasional use or regular therapy, 3-4 times weekly) and the patient’s personal experience. Patients need to know whether a drug is short- or long-acting, possible disadvantages and how to use it Given the lack of adequate head-to-head trials, it is difficult to determine the superiority of one agent over another.
Other uses
Besides use in ED, PDE5 inhibitors are used in benign prostatic hypertrophy and in patients with pulmonary arterial hypertension where they are better than Beraprost. Vardenefil is used in dose of 5mg twice daily. Tadalafil has a label indication for the treatment of lower urinary tract symptoms (LUTS) in men.
| Property | Sildenafil | Tadalafil | Vardenafil | Avanafil |
| >TMAX | 30-120 min (median 60 min) | 30=360 min (median 120 min) | 30-120 min (median 60 min) | Mddian 30-45 min |
| Terminal half-life | 4 h | 17.5 h | 4h | 6-17h |
| Absorption | Fatty meals cause a mean delay in TMAX of 60 min | Not affected by food | Fatty meals cause a reduction in CMAX | Fatty meals cause a minimal reduction in CMAX |
| Available doses | 25mg, 50mg and 100 mg, as required | 2.5 mg or 5 mg daily 5 mg,10 mg and 20 mg as required | 2.5mg, 5 mg, 10mg and 20 mg, as required | 50mg, 100 mg and 200mg, as required |
| Maximum dose | 100 mg | 20 mg | 20mg | 200mg |
| Efficacy | Each of the PDE5i offers similar efficacy | |||
| Dose adjustments that may be needed | • Patients aged >65 • Hepatic impairment • Renal impairment • Concomitant use of potent cytochrome P450 3A4 in-hibitors (eg,ritonavir, co-bicistat and erythromycin) • Concomitant use of cimetidine | • Patients aged >65 years • Hepatics impairments • Renal impairment • Concomitant use of potent cytochrome p450 3A4 inhibitors, such as ritonavir, cobicistat and erythromycin | • Patients aged >65 years • Hepatic impairment • Renal impairment • Concomitant use of potent cytochrome P450 3A4 inhibitors, such as ritonavir, cobicistat and erythromycin | • Patients aged >65 years • Hepatic impairment • Renal impairment • Concomitant use of potent cytochrome P450 3A4 inhibitors, such as ritonavir, cobicistat and erythromycin |
| Contraindications | Any patients using organic nitrates either regularly or intermittently Known hypersensitivity to any component of the tablet | |||
| Use with α-blockers | Concomitant use of selective α=blockers does not present a risk for significant hypotension There is a risk of significant hypotension when using non-selective α-blockers |
| Sildenafil | Vardefanil | Taladafil | Avanafil | |
| Headache | 16% | 16% | 14% | 15% |
| Nausea | 7% | 4% | 10% | 4% |
| Back Pain | - | - | 6% | - |
| Nasal congestion | 4% | 10% | 5% | 10% |
| Muscle Pain | - | - | 5% | - |
| Redness | 10% | 12% | 4% | 10% |
| Vision Disorder | 3% | - | - | - |
Status of drugs
Udenafil is newly developed, potent, selective PDE-5 inhibitor that can also inhibit cyclic guanosine monophosphate hydrolysis. Its pharmacokinetic profile includes unique clinical properties of both a relatively rapid onset and a long duration of action.
Mirodenafil is a newly developed oral PDE-5 inhibitor for the treatment of ED. PDE5 inhibitors continues to be the current therapy of choice, approximately 40% of men treated with PDE5 inhibitors fail to have significant improvement in erectile function.
The results of RCTs have shown that these five PDE- 5 inhibitors are more effective than placebo in improving erectile function in Asian men with ED where the psychological component is more dominant.
Supportive herbal medicine
Many herbs show potential to be effective in improving men’s sexual function, but some evidence actually exists to support the use of any herbal medication in the treatment of ED.
| Name of plant | Common name | Part used |
| Allium sativum L. | Garlic | Bulb |
| Asparagus racemosus Willd | Asparagus | Root |
| Boerhavia diffusa L. | Punarnava | Root |
| Chylorophytum tubersum Baker | Safed musli | Whole plant |
| Cocculs cardifolia Linn. | Guduchi | Stem, leaf , root |
| Fadogia agretis Schweinf. Ex Heim | Black aphrodisiac | Stem |
| Myristica fragrans Houtt | Nutmeg | Seed |
| Panax ginseng | Ginseng | Root |
| Turnera aphrodisiaca | Damiana | Areal part |
| Withania somnifera Linn. | Ashwagandha | Leaf, root |
| Pausinystalia yohimbe | yohimbine | Bark |
| Ginkgo biloba | Ginkgo | Leaves,seeds |
| Tribulus terristeris | Caltrop | Seeds |
| Asphaltum bitumen | Shilajit | Pitch |
| Mucuna pruriens | Kapi kacchu | Seed |
| Asparagus racemosus | Shatawari | Root |
| Erythroxylem catuaba | Catuaba | Bark |
| Ipomoea digitate | Vidari kandha | Root |
| Anacyclus pyrethrum | Akarakarabha | Root |
| Allium tuberosum | Chinese chive | Seed |
Red Korean ginseng and Yohimbine have unknown mechanism of action (possibly act as a nitric oxide donor).
Herbal remedies may have only adjuvant role. The safety and efficacy of herbal remedies have not been assessed, unlike synthetic drugs, well-controlled and randomized studies are warranted to establish the therapeutic efficy and safety of such products.[13]
Table for Herbal Drugs: [Table 4]
Apomorphine SL (Ixense, Uprima).
Sublingual apomorphine is a treatment option for erectile dysfunction.
Centrally-acting dopamine agonist - acts primarily on the D1 and D2 receptors, although it has a degree of selectivity for the latter
Effective after about 20 minutes.
Does not affect sexual desire; only produces an erection with sexual stimulation
It is well tolerated at doses producing a positive response in about 40-50% of patients.
Adverse effects include: headache, nausea, dizziness, syncope
Contraindications include: coronary artery disease, prolonged QT interval, orthostatic hypotension.
More than 5,000 men with erectile dysfunction participated in clinical trials assessing the safety and efficacy of doses ranging from 2 to 6 mg of Apomorphine. The most favorable risk/benefit ratio is seen with a dose-optimization regimen of 2-3 mg: the 3mg dose provides efficacy comparable to that of 4 mg but with fewer side effects. Consequently, review of clinical studies focuses on data with the 2- to 3-mg dose, the registered dose for use in clinical practice. The primary efficacy endpoint in most clinical trials with apomorphine SL was the percentage of attempts resulting in erections firm enough for intercourse - one of the most rigorous endpoints used in ED trials to date.[14]
Recently, much attention has been given to cell or stem cell therapy for the treatment of ED at the preclinical level. Possible challenges for the use of local gene therapy approaches for the treatment of ED are the selection of an ideal vector system that is safe for the patient. The genes therapy are related to either cavernosal relaxation; calcitonin gene-related peptide, growth factors; brain-derived neurotrophic factor (BDNF) and neurotrophic factor, counteraction of oxidative stress such as superoxide dismutase, or inhibition of contractile factors such as rho kinase These are under evaluation.[15]
Second Line Therapy
Alprostadil attenuates presynaptic noradrenaline release in the corpus cavernosum which is essential for the maintenance of a flaccid and non-erect penis. The mechanism of action of alprostadil is targeted at the end organ. Alprostadil acts directly on the penile and vascular smooth muscle cells to stimulate the production of cAMP with resulting intracellular calcium sequestration and subsequent smooth muscle relaxation, penile tumescence, and eventual erection. Alprostadil induces erection by relaxation of trabecular smooth muscle and by dilation of cavernous arteries. Alprostadil (PGE1) is indicated for the treatment of erectile dysfunction due to neurogenic. Patients with sickle cell anemia or trait, leukemia, and tumor of the bone marrow (multiple myeloma) should avoid alprostadil therapy. The dosage range of Alprostadil for the treatment of erectile dysfunction is 1 to 40 mcg.
Alprostadil PGEI (Monotherapy was most effective in psychogenic ED ie (alprostadil–100%, sildenafil–88.9%), least effective in vein occlusive ED (alprostadil–33.3%, sildenafil–22.2%).
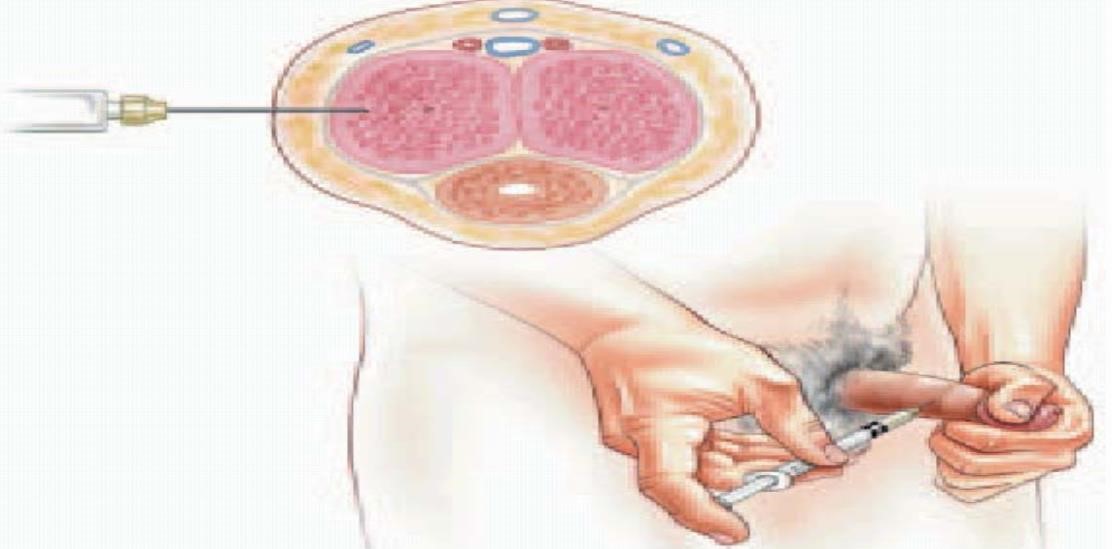
Intracavernosal injections containing phentolamine and papaverine with or without alprostadil are also available.
and eventual erection. Alprostadil induces erection by relaxation of trabecular smooth muscle and by dilation of cavernous arteries. Alprostadil (PGE1) is indicated for the treatment of erectile dysfunction due to neurogenic. Patients with sickle cell anemia or trait, leukemia, and tumor of the bone marrow (multiple myeloma) should avoid alprostadil therapy. The dosage range of Alprostadil for the treatment of erectile dysfunction is 1 to 40 mcg.
Alprostadil PGEI (Monotherapy was most effective in psychogenic ED ie (alprostadil–100%, sildenafil–88.9%), least effective in vein occlusive ED (alprostadil–33.3%, sildenafil–22.2%).
Intracavernosal injections containing phentolamine and papaverine with or without alprostadil are also available.
Patients should be warned about priapism and advised on initial management with moderate exercise and decongestant tablets and to seek medical advice if priapism persists after 4-6 hours. [16][Figure 8]
Caverject vial when injecting the diluent into the sterile powder vial and when removing the correct dose for injection from the Caverject vial). The deliverable amount of alprostadil in these dilutions is 5 mcg/mL, 10 mcg/mL, 20 mcg/mL, or 40 mcg/mL, respectively, because some drug is absorbed onto the vial and syringe.
Intraurethrral Therapy
Alprostadil is used to treat erectile dysfunction (ED) in adult males. The efficacy of alprostadil in treating ED varies with the cause; response rate is generally lower in patients with ED due to mixed etiologies compared to those with ED due to neurogenic, psychogenic, or vasculogenic causes. Two dosage forms are marketed for treating ED: a transurethral product (Muse- Medicated Urethral System for Erections) which uses a medicated pellet administered into the urethra and an injection (Caverject or Edex) that is directly injected into the corpus cavernosa.
Alprostadil (MUSE) is administered as a urethral suppository. Central nervous system adverse reactions of alprostadil are frequently reported. During post- marketing surveillance, syncope occurring within 1 hour of administration has been reported. Local adverse reactions associated with alprostadil used for treating erectile dysfunction were usually mild and transient; however, approximately 7% of patients withdrew from therapy because of adverse reactions. The most frequent local adverse reactions reported with the use of alprostadil urethral suppository include penile pain (36%), urethral pain (13%), and testicular pain (5%).
Alprostadil cream (Vitaros/Virirec)
Combines the efficacy of alprostadil with an ‘easy to use’ formulation. Alprostadil is a synthetic analog of prostaglandin E1 (PGE1), equivalent to naturally occurring PGE1. Its mechanism of action involves the binding to G protein coupled PGE1 receptors localized on the surface of smooth muscle cells, thus activating cAMP (cyclic adenosine monophosphate), which in turn induces penile vascular smooth muscle relaxation to provide penile erection.[17]
Third Line options or Surgical intervention
Implantation of penile prosthesis is indicated for the treatment of organic ED in men who fail or reject more conservative measures, such as oral PDE5 inhibitors, vacuum erection devices (VED), urethral alprostadil suppositories, and intracavernosal injection therapy.
The Vacuum constriction device consists of an acrylic cylinder with a pump that may be attached directly to the end of the penis. A constriction ring or band is placed on the cylinder at the other end, which is applied to the body. The cylinder and pump are used to create a vacuum to help the penis. The adverse effects include penile pain, numbness and delayed ejaculatiom, shown in [Figure 9] [18]
Least invasive method of all
Requires no medication or surgery

Penile prostheses are represented by several constructive models: semirigid rod, positionable, two piece inflatable or three piece inflatable though the cost and high invasiveness of the procedure may reduce its expansion in the general population, the results are generally better, in terms of erection, personal and partner satisfaction.
Penile prosthesis implantation
The important one is the 3 piece system consists of corporal cylinders, a scrotal pump, and a separate reservoir. The 2-piece system eliminates the separate reservoir, instead incorporating it into the proximal aspect of the inflatable cylinders. The scrotal pump moves the saline into distal part the cylinders to provide an erection, shown in.[Figure 10]

Advantages of the Ambicor
Considered easier to deflate: bending the penis vs. the fine motor skills and strength necessary to locate and press the pressure release area on the scrotal pump found in the 3-piece device.
Potentially easier to inflate, with only 3 to 6 pumps typically necessary.
With no separate reservoir in the Ambicor, the reservoir placement causing potential injury to the bowel, bladder, or vessels can be avoided.
Totally hidden and concealed within the body.
Natural flaccidity compared to non-inflatable implant.
Less parts and therefore less chance of mechanical failure.
Disadvantages of implants
Once an implant has been placed, natural erections usually no longer occur. If the prostheses were then removed the normal erections are unlikely to return. There is a small chance of infection which would require removal of the prosthesis. Some patients can develop surgical complications or anesthetic complications.
2.2. Complications: urethral and corpus cavernosa perforation
The main surgical procedures used today are penile revascularization and penile venous surgery, recommended only for selected patients and offering fair long-term results.[19], [20]
Conclusion
ED is a multifaceted condition that may involve any one or more of several different organic causes. These may belong to the vascular, hormonal or nervous system, or a combination of more than one of them. Conversely, psychogenic ED is the result of psychological factors that reduce an individual’s sexual responsiveness and desire. This is fairly common in Asian population.
Pharmacotherapy may prove to be highly effective in the management of organic ED. The oral PDE5 inhibitors are the current first-line treatment options of choice. Penile prosthesis implantation is currently the most effective treatment option in terms of both patient and partner satisfaction in the management of ED. Satisfaction rates and prosthesis survival significantly increased with the improvements in both prosthesis design and surgical techniques. A study published in May 2014 in The Journal of Sexual Medicine found that some percentage of men can reverse erectile dysfunction with healthy lifestyle changes, such as exercise, weight loss, a varied diet, and good sleep. The Australian researchers also showed that even if erectile dysfunction medication is required, it's likely to be more effective if one can implement these healthy lifestyle changes.
Source of Funding
None.
Conflict of Interest
None.
References
- Monica G. Ferrini, Nestor F. Gonzalez-Cadavid, Jacob Rajfer. Aging related erectile dysfunction—potential mechanism to halt or delay its onset. Transl Androl Urol 2017. [Google Scholar]
- . [A] Salman M, Erectile dysfunction: prevalence, risk factors and involvement of antihypertensive drugs intervention Trop J Pharm Res 2016;15(4):869-76 4[B] Cheng JYW. Prevalence of erectile dysfunction in Asian populations: a meta-analysis. Int J Impot Res 2007;19:229–44. . [Google Scholar]
- Pietro Gareri, Alberto Castagna, Davide Francomano, Gregorio Cerminara, Pasquale De Fazio. Erectile Dysfunction in the Elderly: An Old Widespread Issue with Novel Treatment Perspectives. Int J Endocrinol 2014. [Google Scholar]
- . https://www.healthline.com/health/what-sexual-dysfunction. . [Google Scholar]
- Geng-Long Hsu. The venous drainage of the corpora cavernosa in the human penisArab. J Urol 2013. [Google Scholar]
- Kenia Pedrosa Nunes, R. Clinton Webb. Mechanisms in Erectile Function and Dysfunction: An Overview. 2012. [Google Scholar]
- I F Ghalayini. Nitric oxide–cyclic GMP pathway with some emphasis on cavernosal contractility. Int J Impotence Res 2004. [Google Scholar]
- Asif Muneer. Urology News. 2013. [Google Scholar]
- A Marais. The pharmacological management of erectile dysfunction. J Endocrinol, Metab Diabetes South Afr 2015. [Google Scholar]
- N Schellack, G Schellack. The management of erectile dysfunction. S Afr Pharm J 2013. [Google Scholar]
- Jacob Rajfer. Relationship Between Testosterone and ErectileDysfunction, Review in Urology . Spring 2000. [Google Scholar]
- . 12.[A] Huang SA, Janette D. Lie, Phosphodiesterase-5 (PDE5) Inhibitors In the Management of Erectile Dysfunction, Drug class review 2013;38(7) [B] Bourin M, Clinical Pharmacology of Phosphodiesterase 5 Inhibitors in Erectile Dysfunction SOA. Arch Pharm Pharmacol, 20031(1).. . [Google Scholar]
- Ashwin Saxena, Pawan Prakash, Mayur Porwal, Neeraj Sissodia. Pravesh Sharma Erectile dysfunction: A review and herbs used for its treatmentInternational. J Green Pharm 2012. [Google Scholar]
- Paul Arduca. Erectile Dysfunction: A guide to diagnosis and management. Middle East J Family Med 2004. [Google Scholar]
- Ji-Kan Ryu. Kyu SuhTherapeutic Angiogenesis as a Potential Future Treatment Strategy for Erectile Dysfunction. World J Mens Health 2012. [Google Scholar]
- Chistopher G Mcmohan. Current diagnosis and management of erectile dysfunction. Med J Aus 2019. [Google Scholar]
- . https://www.webmd.com/drugs/2/drug-. . [Google Scholar]
- Paul Arduca. Erectile dysfunction. Australian Family Physician 2003. [Google Scholar]
- Susanne A Quallich, Dana A Ohl. Penile Prosthesis: Patient Teaching and Perioperative Care. Urol Nur 2002. [Google Scholar]
- Faruk Kucukdurmaz, Ates Kadioglu. Surgical Treatment of Erectile Dysfunction - Disease-Associated Mechanisms and Novel Insights into Therapy. 2012. [Google Scholar]
- Introduction
- Erectile dysfunction
- Male menopause or Andropause
- Prevalence
- Basics of Penile erection
- Physiology of Penile erection
- Diagnosis of Erectile Dysfunction
- Treatment options for erectile dysfunction conservative medical therapy
- Treatment Algorithm for Erectile Dysfunction
- First Line Therapy
- Properties of oral 5 phosphodiesterase inhibitors [[12] A]
- Mode of action
- Pharmacodynamics
- Relative safety of Vardenafil (BAY 38-9456) & Avanafil(Stendra)
- Relative activity
- Choice of drug
- Other uses
- Status of drugs
- Supportive herbal medicine
- Second Line Therapy
- Intraurethrral Therapy
- Alprostadil cream (Vitaros/Virirec)
- Third Line options or Surgical intervention
- Penile prosthesis implantation
- Advantages of the Ambicor
- Disadvantages of implants
- 2.2. Complications: urethral and corpus cavernosa perforation
- Conclusion
- Source of Funding
- Conflict of Interest