- Visibility 893 Views
- Downloads 1k Downloads
- Permissions
- DOI 10.18231/j.agems.2024.011
-
CrossMark

A true experimental study to assess the effectiveness of juice in relieving constipation among older adults in a selected hospital, Kolar
- Author Details:
-
 Vani R *
Vani R *
-
Zeanath Cariena Joseph
-
Abiya
-
Aleena
-
Akhila
-
Algeena
-
Tinu
-
Namitha
-
Suma
-
Treesa
-
Usha
-
Treesa Saji
-
Adithya
-
Abhilash
Abstract
Introduction: Chronic constipation becomes more common as people age, in both genders, although it becomes most common beyond age 60. Aloe vera is commonly used as a potent laxative and as a substance to enhance gastrointestinal motility. Aloe vera can be used as a natural remedy for constipation at affordable prices among old age people.
Aims and Objective: Study aimed to assess the effectiveness of aloeAloe vera juice to relieve constipation among older adults.
Materials and Methods: For the present study, a randomized control trial pretest-posttest design was adopted. Subjects consist of 60 (30 Experimental and 30 Control) older adults from R.L. Jalappa Hospital and Research Centre. The pretest was conducted using the Constipation Assessment Scale (CAS) through the Block Randomization sampling technique in both groups. A freshly prepared Aaloe vera juice of 100 milligrams per day was given for 20 days. Posttest was conducted in both experimental and control group after 10th, and 20th day. The data gathered were analyzed by descriptive and inferential statistical method using frequency, percentage, SD, Independent t test, paired t test and RMANOVA with Posthoc test.
Results: The dataset comprised 60 elderly patients. In total, the Majority of respondents 70% and 73.3% reported moderate level constipation in the experimental group & and control group during pretest. Constipation scores of no problem during posttest-I was 93.3% & 96% in experimental group during 10th and 20th day. Whereas in control group remains unchanged with moderate and severe constipation scores. Independent “t”test and RMANOVA found to be significant in experimental group.
Conclusion: Constipation remains a clinical problem among elderly. There is a significant relationship between effectiveness of Aaloe vera juice in relieving constipation among old age people. Furthermore study emphasize that, home remedy based laxatives which are affordable, available aloevera Aloe vera juice are effective to relive constipation among elderly.
Keywords: Aloe vera, Constipation, Old Age
Introduction
Aloe vera is widely used as a strong laxative and to promote gastrointestinal motility. Aloe vera treatment may be beneficial for patients with constipation-predominant irritable bowel syndrome or functional constipation.[1] It may be used as a natural remedy for constipation and eaten in a juice, gel, or tablet form. When constipated, aloe Aloe latex is mostly administered orally to help the intestines spontaneously empty.[2] As a result, osmotic laxatives and lifestyle modification stimulants are the primary therapy in the management algorithm.[3]
Persistent constipation appears to be somewhat frequent among people in general.[4] According to estimates, between 2% and 28% of Indians experience chronic constipation; the majority of estimates range between 12% and 19%. Depending on the diagnostic criteria, its occurrence varies.[5] Chronic constipation disproportionately affects women (2:2:1), and as people age, the incidence has increased.[6]
One study found that elderly people who consume less calories and meals are also more likely to become constipated.[7] Comorbid diseases and residing in a care facility are two possible risk factors for constipation.[8]
Constipation is a common issue and challenge for the elderly. Constipation increases with age and is environment-related.[9] The incidence is 26% for women and 26% for males among community members 65 years of age or older; the greatest rate is found among individuals 84 years of age or older. It may affect as many as 80% of residents in long-term care settings.[10]
Hence, the investigator has decided to manage constipation by using home remedial measures with affordable prices among old age people with use of aloe Aloe vera. Because it is one of easily available medicinal aloe Aloe vera and had got many medicinal effects.
Materials & Methods
After obtaining the institutional ethics committee approval (CTRI/2023/11/059828), a single-blinded randomized control trial study was conducted among the elderly in a tertiary care Hospital from September to November 2023. Volunteer inclusion criteria were adults aged≥ 60 years, seeking medical services at IPD, able to speak and understand Kannada or English, and accessible for follow-up throughout the study period by providing written consent. Participant recruitment of older adult’s aged ≥60 years who are seeking medical services at R.LJ. Hospital and Research Centre, Tamaka, Kolar. (n=30) in the Experimental group and Control group (n=30), were recruited by using a Block randomization technique. The experimental group was given aloevera Aloe vera juice whereas the Control group received Routine care. Geriatric clients with co-morbid conditions of cardiovascular disorders and Diabetes were excluded. Participant information sheets and written consent forms were given to older adults which were translated in the regional language upon returning the consent forms, participants were invited to attend the study for one month. A sample size of 60 participants was chosen in line with previous sample size recommendations of feasibility studies.
Setting of the study
Tertiary Care hospital, at R.L. Jalappa Hospital and Research Centre, Tamaka, Kolar.
Sample size
derived by employing the Med. Calc statistical software assessed the difference between the two means as 14.2 and the SD or variance of 22.7 with the effect size of 0.2, with a 80% power of the study and a predetermined significance level of 95% (CI) with a two-tailed test and 5% absolute precision alpha error (d) and assuming 10% to be an attrition rate the estimated sample size was around 25 in each group. If 10% of the sample's dropouts were taken into account, the estimated sample size was around 30 in each group
Considering the Cochran’s formula
n =2(Zα +Z 1-β)2 σ2d2Zα= 95% Confidence Interval β) = Power of the study as 80%
σ2 Average variance estimation d = Effect size.
Sampling technique
Block randomization where wards have been categorized using Rraosoftware into blocks of 4x4 and the blocks were classified based on Block A as experimental group & Block B as control group.
Data collection tools
The tool was prepared based on the research problem, objectives of the study stated were assessed by using standardized Constipation Assessment Scale (CAS).[11]
Section-I: Proforma on Sociodemographic variables: age, gender, marital status, Educational qualification, Type of family, Co-morbidities, Health checkups undergone, and Bio physiological parameters were assessed such as Nutritional status, Vision, hearing acuity, Sleep pattern, Bowel & Bladder pattern, Physical activity per day, were recorded to provide participants’ baseline characteristics. It is shown in the [Table 2].
Section II: McMillan and Williams (1989) Standardized Eight item “Constipation Assessment Scale” used on old age people who have constipation. represented in the [Table 3], [Table 4], [Table 5].
Intervention
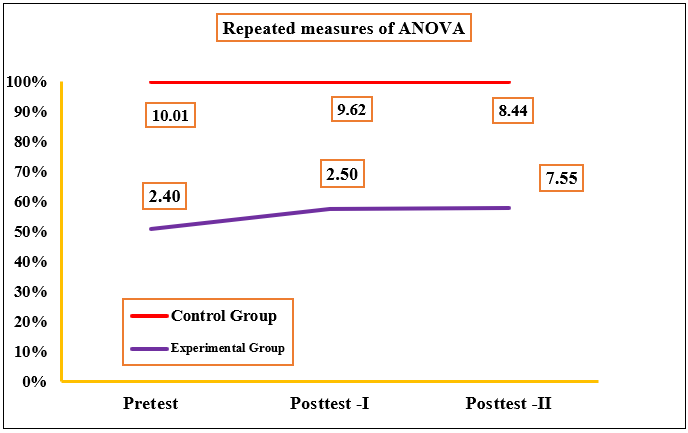
Add 5ml-10ml of aloe Aloevera gel of 100 milligrams per day and Mix with 100 ml of water. Each day, 2 inch portions of aloe Aloe vera gel along with 1 cup of water to a blender were added. Blend only for 30 to 60 seconds until the aloe Aloe vera gel is fully crushed. Each day fresh juice is prepared and served to experimental group till 20 days and posttest assessed on 10th and 20th day.[12], [13], [14], [15] RMANOVA Performed to assess the effectiveness of aloevera juice represented in [Figure 1].
|
Data analysis |
||
|
Methods |
Type of Statistics |
Purposes |
|
Descriptive Statistics |
Frequency, Percentage, Mean, SD |
Participants socio-demographic characteristics |
|
Inferential Statistics |
Paired ‘t’ test |
Compare the outcome variables before and after intervention within the group |
|
Independent ‘t’ test |
Compare the outcome variables before and after Intervention between the groups |
|
|
Repeated Measures of ANOVA |
Assess differences in outcome over time. |
|
|
Chi-square |
Find an association of selected socio-demographic variables with outcome variables |
|
Sl.no |
Demographic Variables |
Category |
Study groups f (%) |
df |
χ² & (p value) |
|
|
Experimental |
Control |
|||||
|
1. |
Age (in Years) |
60-70 |
27 (90) |
20 (66.6) |
2 |
Fisher exact test 0.0575. NS p > .05. |
|
71-80 |
3 (10) |
10 (33.3) |
||||
|
2. |
Gender |
Male |
17 (56.6) |
18 (60) |
1 |
χ²= 0.068 (.793) NS p > .05. |
|
Female |
13 (43.3) |
12 (40) |
|
|||
|
3. |
Educational status |
Formal education |
16(53.3) |
17 (56.6) |
1 |
χ²= 0.078 (.551) NS p > .05 |
|
No formal education |
14 (46.6) |
13 (43.3) |
|
|||
|
4. |
Religion |
Hindu |
24 (80) |
23(76.6) |
1 |
χ²=0.098 (.754) NS p > .05. |
|
Muslim |
6 (20) |
7 (23.3) |
|
|||
|
5. |
Marital Status |
Married |
22 (73.3) |
24 (80) |
1 |
χ²=0.372(.541) NS p > .05. |
|
Widowed/widower |
8(26.6) |
6(20) |
|
|||
|
6. |
Place of Residence |
Rural |
23 (76.6) |
22 (73.3) |
|
χ²= 0.088(.765) NS p > .05. |
|
Semi-urban/ Urban |
7 (23.3) |
8 (26.6) |
1 |
|||
|
7. |
Socio-economic Status |
APL |
6(20) |
5(16.6) |
1 |
χ²= 0.111 (.738) NS p > .05 |
|
BPL |
24(80) |
25 (83.3) |
|
|||
|
8. |
Type of Family |
Nuclear Family |
26 (86.6) |
23 (76.6) |
1 |
χ²=1.00(.316) NS p > .05. |
|
Joint Family |
4 (13.3) |
7 (23.3) |
|
|||
|
9. |
Nutritional Status |
Under-weight |
19 (63.3) |
18 (60) |
2 |
χ²=0.451 (.798) NS p > .05. |
|
Normal weight |
6 (20) |
5 (16.6) |
|
|||
|
Overweight / Obese |
5 (16.6) |
7 (23.3) |
|
|||
|
10 |
Sleeping Pattern |
Normal /Adequate |
21 (70) |
22 (73.3) |
1 |
χ²=0.082 (.774) NS p > .05 |
|
Disturbed/Inadequate |
9 (30) |
8 (26.6) |
|
|||
|
11 |
Bowel |
Regular |
5 (16.6) |
9 (30) |
1 |
χ²=1.490(.222) NS p > .05 |
|
Irregular |
25 (83.3) |
21 (70) |
|
|||
|
12 |
Bladder |
Normal |
25 (83.3) |
24 (80) |
1 |
χ²= 0.111(.738) NS p > .05. |
|
Urinary Incontinence |
5(16.6) |
6 (20) |
|
|||
|
13 |
Physical Activity Performed Per day |
Not Involved |
17 (56.6) |
12 (40) |
1 |
χ²=1.668(.196) NS p > .05 |
|
Low |
13 (43.3) |
18 (60) |
|
|||
|
Sl. no |
Severity of constipation |
Score range |
Experimental group f (%) |
Control group f (%) |
||||
|
Pretest |
Posttest-1 |
Posttest-2 |
Pretest |
Posttest-1 |
Posttest-2 |
|||
|
1. |
No Problem |
0-5 |
8 (26.6) |
28(93.3) |
29(96.6) |
3 (10) |
2 (6.6) |
1(3.3) |
|
2. |
Some Problem |
6-10 |
21(70) |
2 (6.6) |
1 (3.3) |
22(73.3) |
20(73.3) |
27(90) |
|
3. |
Severe Problem |
11-16 |
1(3.3) |
0(0) |
0(0) |
5(16.6) |
8(16.6) |
2(6.6) |
|
|
Total |
30 |
30 |
30 |
30 |
30 |
30 |
|
Sl.no |
Severity of constipation at time of test |
Experimental group |
Control group |
MD |
Independent ‘t’ Value |
p-Value & Inference |
|
Mean ± SD |
||||||
|
1. |
Pretest |
7.55 ±1.94 |
8.44 ± 1.58 |
5.05 |
6.88 |
.212 NS |
|
2. |
Posttest 1 |
2.50 ±0.75 |
9.62± 2.13 |
1.18 |
1.30 |
<0.001**SS |
|
3. |
Posttest 2 |
2.24±0.69 |
10.01± 2.24 |
7.77 |
1.21 |
<0.001** SS |
|
Sl.no |
Demographic Variables |
Experimental |
Control Group |
||||
|
Below Median (<8) |
Above Median (>8) |
χ2 &p value |
Poor<18 |
M.P(>26) |
χ2 &p value |
||
|
1. |
Age |
|
|
χ2=0.475(.490) NS p > .05 |
|
|
χ2=0.002 (.960.) NS p > .05. |
|
a. b. |
60-70 years 71-80 years |
7 7 |
10 6 |
8 6 |
9 7 |
||
|
2. |
Gender |
|
|
χ2=0.135(.7125) NS p > .05 |
|
|
χ2= 0.002 (.960.) NS p > .05. |
|
a. |
Male |
7 |
8 |
9 |
6 |
||
|
b. |
Female |
6 |
9 |
8 |
6 |
||
|
3 |
Educational status |
|
|
χ2=0.475 (.490) NS p >.05. |
|
|
χ2= 0.002 (.960.) NS p > .05. |
|
a. |
Formal education |
6 |
10 |
9 |
8 |
||
|
b. |
No formal education |
7 |
7 |
7 |
6 |
||
|
04 |
Religion |
|
|
χ2=0.002(.960) SS p > .05. |
|
|
χ2= 0.143 (.704.) NS p > .05. |
|
a. |
Hindu |
9 |
10 |
10 |
9 |
||
|
|
Other religion |
5 |
6 |
|
5 |
6 |
|
|
05 |
Marital status |
|
|
χ2=0.143 (.704) NS p > .05. |
|
|
χ2=1.221 (.269.) NS p > .05. |
|
a. |
Married |
10 |
5 |
7 |
8 |
||
|
b. |
Widower/ widow |
9 |
6 |
10 |
5 |
||
|
06 |
Place of Residence |
|
|
χ2=1.832(.175.) NS p > .05. |
|
|
χ2= 0.535 (.464.) NS p > .05. |
|
a. |
Rural |
12 |
6 |
8 |
6 |
||
|
b. |
Semi-urban |
6 |
6 |
7 |
9 |
||
|
07 |
Socioeconomic status |
|
|
χ2=0.010.(.919.) NS p > .05. |
|
|
χ2= 0.133. (.715.) NS p > .05. |
|
a. |
APL |
9 |
5 |
8 |
7 |
||
|
b. |
BPL |
10 |
6 |
7 |
8 |
||
|
08 |
Type of family |
|
|
χ2=0.153.(.695. ) NS p > .05. |
|
|
χ2= 3.096. (.078.) NS p > .05. |
|
a. |
Nuclear Family |
8 |
6 |
12 |
5 |
||
|
b. |
Joint Family |
8 |
8 |
5 |
8 |
||
|
09 |
Nutritional status |
|
|
χ2=0.833.(.361.) NS p > .05. |
|
|
χ2=0.271.(.602.) NS p > .05 |
|
a. |
Underweight/obese |
6 |
6 |
12 |
5 |
||
|
b. |
Normal weight |
6 |
12 |
8 |
5 |
||
|
10 |
Sleep Pattern |
|
|
χ2=0.535. (.464.) NS p > .05. |
|
|
χ2=0.002.(.960.) NS p > .05. |
|
a. |
Normal/Adequate |
9 |
7 |
9 |
7 |
||
|
b. |
Disturbed/Inadequate |
6 |
8 |
8 |
6 |
||
|
11. |
Bowel |
|
|
|
|
|
|
|
a. |
Regular |
5 |
10 |
χ2=0.143.(.704.) NS p > .05. |
10 |
6 |
χ2= 2.142. (.143.) NS p > .05. |
|
b. |
Irregular |
6 |
9 |
5 |
9 |
||
|
12. |
Bladder |
|
|
|
|
|
|
|
a. |
Normal |
9 |
8 |
χ2=0.135.(.712.) NS p > .05 |
9 |
8 |
χ2=0.002.(.960.) NS p > .05. |
|
b. |
Urinary Incontinence |
6 |
7 |
7 |
6 |
||
|
13. |
Physical activities performed per day |
|
|
|
|
|
|
|
a. |
Not involved |
6 |
10 |
χ2=1.157.(.281. ) NS p > .05. |
12 |
6 |
χ2=2.424.(.119.) NS p > .05. |
|
b. |
Low |
8 |
6 |
5 |
8 |
||
|
14. |
If you fall sick, do you prefer to go |
|
|
|
|
|
|
|
a. |
Hospital Treatment |
9 |
6 |
χ2=0.135.(.712. )NS p > .05. |
11 |
6 |
χ2=1.032.(.309.) NS p > .05. |
|
b. |
With medicines |
8 |
7 |
6 |
7 |
||
|
15. |
Source of information |
|
|
|
|
|
|
|
a. |
Mass Media |
9 |
7 |
χ2=0.001.(.960.) SS p > .05. |
9 |
7 |
χ2= 0.002(.960). NS p > .05. |
Results
[Table 3] depicts the frequency and percentage distribution of constipation assessment among older adults during pretest and posttest, with significant improvements after the intervention.
[Table 4] depicts the mean scores of constipation assessmentamong older adults during pretest and posttest, with significant improvements after the intervention.
Discussion
It was feasible and safe to deliver a Aloe vera juice Intervention among geriatric clients in health care and community settings.[16] The intervention was acceptable to Geriatric clients, Caretakers and it can be developed as a protocol to improve health promotion outcome measures among the elderly.[17] A key to success was the availability &medicinal effects of Aaloe vera juice to improve their Quality of Life and confidence to engage with the home remedial measures.[18] This study adds to a growing body of evidence that suggests volunteers can successfully provide a intervention and take on more direct roles in supporting older individuals.[19]
A systematic review of 21 studies found evidence suggesting that Aloe vera is essential to improve the bowel pattern and improve health outcomes of community-dwelling older adults including severe constipation, Nutritional status[20] On the initial day of recruitment, the participants were given Pretest, followed by an Aloe vera juice Intervention focusing on Constipation assessment. Posttest 1& and posttest 2 on the 10th , 20th day, which showed a greater significant improvement in relief of constipation scores among geriatric clients.[21] Similarly, a range of studies emphasized physical and nutritional aspects in this study holistic comprehensive health promotion measures required for the elderly have been focused.[22]
LeiA systematic review of Aaloe vera and its effectiveness was conducted to synthesize existing research on the relationship between older adults’ health and functioning.[23] A systematic search was conducted of electronic databases (MEDLINE, EMBASE, Biosis, and the Cochrane Library). The study highlighted there are promising results, clinical effectiveness of oral a Aloe vera to relieve constipation among geriatric.[24]
Conclusion
Based on the study findings, Aloe vera is proven to be effective to relieve constipation among older adults. This study demonstrated that it was feasible and safe to deliver a Aloe vera juice for community-dwelling older adults both in hospital and community settings.[25] The geriatric population was found to be the biggest beneficiary of Aloe vera juice intervention strategies as home remedial measures with medicinal effects.[26]
Limitations and scope
The study was conducted among older adults between 60-75 years age group. It can be conducted in community settings. Geriatric population was the biggest beneficiaries. Further research is needed to better understand factors that influence participants’ adherence to intervention strategies to promote the healthy aging.[27]
Nursing implications
Nursing practice: Nursing professionals working in the hospital as well as in the community setup should know how to assess the risk of constipation.
Nursing education: abundant opportunities to educate the elderly about healthy life styles and risk factors of constipation.
Nursing administration: manage the patient care and delivery of specific nursing services within the health care agency.[28]
Nursing research: Nursing research is urgently needed to improve the health with home remedial measures which are proven to be effective.[29] [(30])
Recommendations of the Study
A similar study can be replicated on a large sample in different types of setting.
Source of Funding
None.
Conflict of Interest
None.
Acknowledgment
We would like to acknowledge the tremendous contribution of the all the geriatric clients for the cooperation in conducting the research. We thank all the authorities for the permitting to conduct research . remaining authors who have constantly supported the project from the initial phase of the study till the end in data collection process to Ms. Abiya Shibu, Ms. Namitha Elza Jojo, Ms. Adithya Murali, Ms. Suma.A,Ms. Akhila.A, Ms. Tessa Saji, Ms. Jinu Jojo, Ms. Aleena Biju, Ms. Treesa Benny, Ms. Algeena Jacob, Ms. Usha L.S, Mr. Abhilash.R, III year BSc(N) students, SDUCON.
References
- Sartorius N. The meanings of health and its promotion. Croat Med J. 2006;47(4):662-4. [Google Scholar]
- Jayanthi P, Ranganathan J. Ageing and its implications. J Oral Maxillofac Pathol. 2010;14(2):48-51. [Google Scholar]
- . National Institute on Ageing: Strategic Directions for Research. Understanding the Dynamics of the Ageing Process. . . [Google Scholar]
- Meika F, Duncan H, Samir S. . Evaluation of the Nutritional and Metabolic Effects of Aloe vera. Herbal Medicine: Biomolecular and Clinical Aspects. . [Google Scholar]
- Elizabeth M. onstipation: Evaluation and Management. Mo Med. 2018;115(3):236-41. [Google Scholar]
- Seung W, Jaeyoung C, Sunmin P, Hyun J, Jong P. Aloe vera is effective and safe in short-term treatment of irritable bowel syndrome: A systematic review and meta-analysis. J Neurogastroenterol Motil. 2018;24(4):528-35. [Google Scholar]
- Glia A, Lindberg G. Quality of life in patients with different types of functional constipation. Scand J Gastroenterol. 1997;32(11):1083-9. [Google Scholar]
- Koloski N, Jones M, Wai R. Impact of persistent constipation on health-related quality of life and mortality in older community-dwelling women. Am J Gastroenterol. 2013;108(7):1152-8. [Google Scholar]
- Drossman D, Sandler R, Mckee D, Lovitz A. Use of a questionnaire to identify a population with bowel dysfunction. Gastroenterology. 1982;83(3):529-34. [Google Scholar]
- Talley N, Keefe E, Zinsmeister A, Melton L. Prevalence of gastrointestinal symptoms in the elderly: a population-based study. Gastroenterology. 1992;102(3):895-901. [Google Scholar]
- Talley N, Fleming K, Evans J. Constipation in an elderly community: a study of prevalence and potential risk factors. Am J Gastroenterol. 1996;91(1):19-25. [Google Scholar]
- Wald A, Scarpignato C, Mueller-Lissner S. A multinational survey of prevalence and patterns of laxative use among adults with self-defined constipation. Aliment Pharmacol Ther. 2008;28(7):917-30. [Google Scholar]
- Sandler R, Jordan M, Shelton B. Demographic and dietary determinants of constipation in the US population. Am J Public Health. 1990;80(2):185-9. [Google Scholar]
- Everhart J, Go V, Johannes R. A longitudinal survey of self-reported bowel habits in the United States. Dig Dis Sci. 1989;34(8):1153-62. [Google Scholar]
- Whitehead W, Drinkwater D, Cheskin L. Constipation in the elderly living at home. Definition, prevalence, and relationship to lifestyle and health status. J Am Geriatr Soc. 1989;37(5):423-9. [Google Scholar]
- Donald I, Smith R, Cruikshank J. A study of constipation in the elderly living at home. Gerontology. 1985;31(2):112-8. [Google Scholar]
- Harari D, Gurwitz J, Avorn J. Bowel habit in relation to age and gender. Findings from the National Health Interview Survey and clinical implications. Arch Intern Med. 1996;156(3):315-20. [Google Scholar]
- Choung R, LG, Schleck C. Cumulative incidence of chronic constipation: a population-based study 1988-2003. Aliment Pharmacol Ther. 2007;26(11-12):1521-8. [Google Scholar]
- Ruby C, Fillenbaum G, Kuchibhatla M, Hanlon J. Laxative use in the community-dwelling elderly. Am J Geriatr Pharm. 2003;1(1):11-7. [Google Scholar]
- Shi L, Wu Y. Epidemiology of constipation in elderly people in part of China: A Multicenter Study. J Res Rev. 2022;10. [Google Scholar]
- Jaeyoung C. Aloevera in effective and safe in short term treatment of irritable bowel syndrome: A Systematic study. J Neurogastro Motil. 2018;76(1):37-51. [Google Scholar]
- Shebi S, Preetha S. Effects Of Aloe Vera On Constipation. J Res Rev Int J Curr Adv Res. 2017;6:1-4. [Google Scholar]
- Red K. Herbal formula improves upper and lower gastrointestinal symptoms and gut health an Australian adults with digestive disorder. J Res Rev. 2020;76:37-51. [Google Scholar]
- Odes H, Madar Z. A double-blind trial of a celandin, aloevera and psyllium laxative preparation in adult patients with constipation. . Digestion. 1991;49(2):65-71. [Google Scholar]
- Prathiba S. Effect of aloe vera syrup on constipation among cancer patients receiving morphine. . Tirumala Coll Nurs. 2023;7(1):23-37. [Google Scholar]
- Fong F, Smit I, Setshedi M, Engel M. Consumption of aloe vera to improve health outcomes in adults with irritable bowel syndrome: A systematic review and meta-analysis. J South Afr Gastroenterol Rev. 2002;20(1):1-5. [Google Scholar]
- Ashafa A, Sunmonu T, Abass A, Ogbe A. Laxative potential of the ethanolic leaf extract of Aloe vera (L.) Burm. f. in Wistar rats with loperamide-induced constipation. J Nat Pharma. 2011;2(3):158-62. [Google Scholar]
- Odes H, Madar Z. A double- blind trial of a celandine ,Aloe Vera and psyllium laxative preparation in adult patients with constipation. J Res Rev Front Gastrointestinal Res. 2009;49(2):1-2. [Google Scholar]
- Foster M, Hunter D, Samman S. Evaluation of the nutritional and metabolic effects of Aloe vera. Herbal Medicine: Biomolecular and Clinical Aspects. 2011. [Google Scholar]